The following interview has been edited for clarity. The original interview can be found here on our YouTube channel.
Dr Liz Corcoran: Hello and welcome everyone to our conversation with Dr Greenland. I am Dr Liz Corcoran from the Down’s Syndrome Research Foundation UK. We are the UK’s medical research charity for people with Down syndrome. This year is our thirtieth birthday: we formed thirty years ago. I’m so excited that we can talk about this research. Katie: please tell us about who you are and what university you work with.
Dr Katie Greenland: Thank you so much for having me, Liz. My name’s Katie Greenland. I work at the London School of Hygiene and Tropical Medicine, and I’m in the International Centre for Evidence in Disability Research.
Dr Liz Corcoran: Thanks for joining me today. Let’s talk today about the study that we funded, which was looking at menstruation in young women and girls with Down syndrome. I’m going to kick off with some questions. Menstruation among teenage girls with Down syndrome: what first led you to investigate this topic, and why do you think this topic is so overlooked?
Dr Katie Greenland: I chose to work on menstrual health because I was hearing so many different things about it. Lots of mums with daughters who are approaching menarche (which is the first period) were really worried. I was hearing people say, ‘what’s going to happen? How’s she going to cope?’ And then I heard other people saying, ‘I’ve heard it’s not really a problem. I don’t think people really have a problem’. So I wondered: what’s true, and who is it true for? And what’s the range of experiences? The more I started looking into it, I realised there were a lot of knowledge gaps.
The first thing we needed to do was simply describe the range of menstrual health experiences and challenges that our young people are facing, as well as their families: and then we can better understand if anything needs to be done to improve their menstrual health. You asked why I think this topic’s been overlooked. Menstrual health was overlooked as a topic in general, until quite recently. It’s a women’s health problem. There’s a lot of stigma around menstrual health, but these things are gradually changing, and there has been a lot more attention and research about menstrual health. But evidence on menstrual health of people with disabilities is much more limited.
The research that’s out there is quite outdated and describes things like sterilisation: there’s not much current research out there. Why? The more general answer is that people with disabilities are generally underserved and under-researched in health, for many reasons. They have barriers to accessing healthcare. There are also a lot of assumptions made about capacity and whether people can provide informed consent, which is necessary for research studies. If people are not used to working with people with disabilities, or if they fear that underlying conditions or medications might complicate how they would interpret their data, often they just exclude them altogether.
Dr Liz Corcoran: What was unique about your research project and the methods that you used?
Dr Katie Greenland: It was simple in many ways because we did a national survey – an online survey of caregivers – and we followed that up with a series of interviews with young people, and with their families, and with their professional caregivers.
I think what was unique about this was that it’s current. There’s not very much recent research being done at all. Also, most of the research out there does not include the direct voice of people with disabilities. In this case, people with Down syndrome, and teenagers. We also had an Advisory Group, which was comprised of young women with Down syndrome, and caregivers of people with Down syndrome, as well as medical professionals. I think the combination of those things meant that we were able to ask relevant questions that mattered to the community.
Then during the interviews, we made sure that we used a lot of participatory methods, to ensure that we were able to learn from the young people as much as we could.
(Article continues after the image)
Dr Liz Corcoran: Wonderful. We found the element of co-production being there from the beginning in this study really compelling. What were the biggest challenges or concerns that carers and families described during your research?
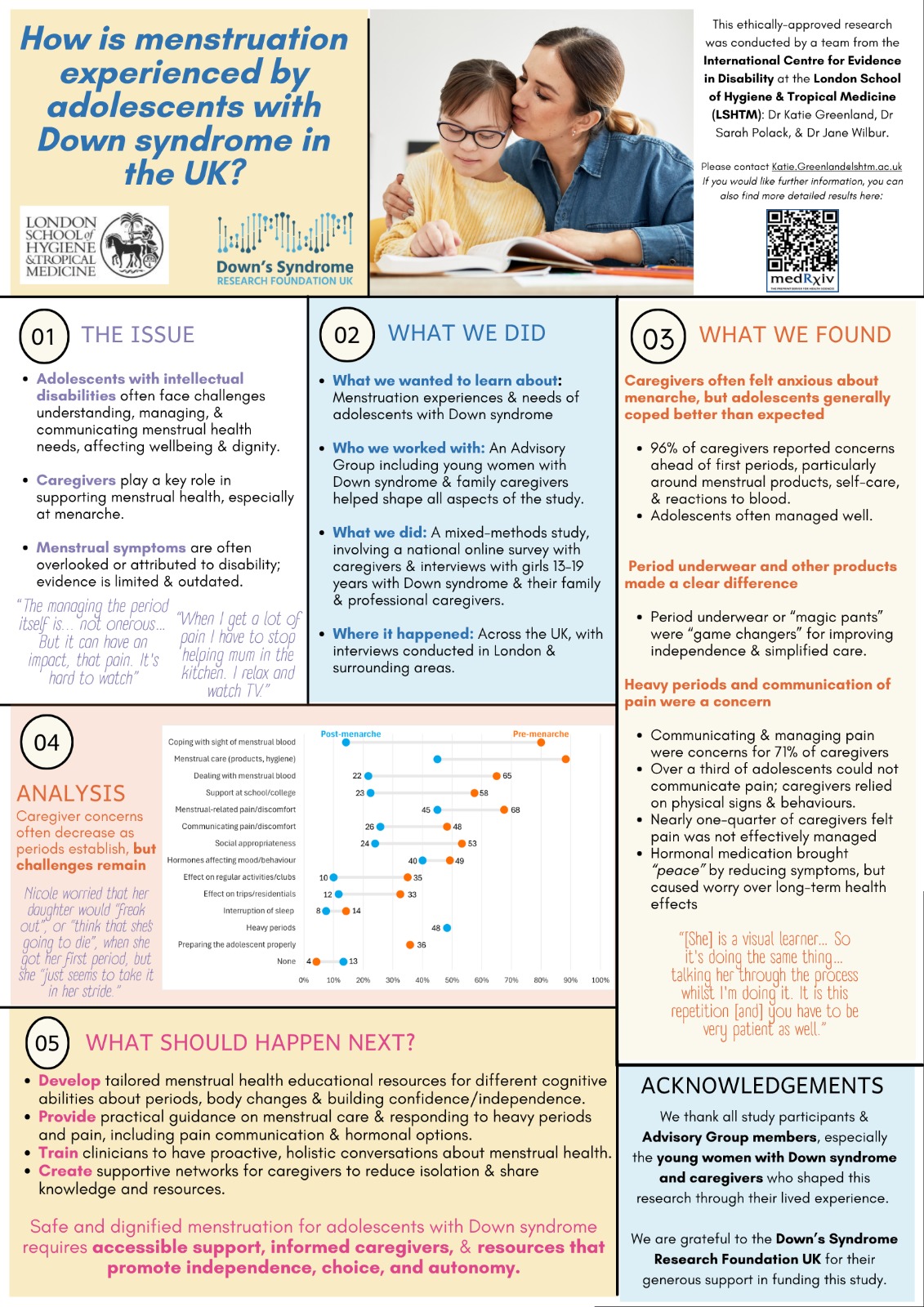
Dr Katie Greenland: We asked them about premenarche (before their daughter got their first period), and then about current experiences. Premenarche, about ninety-six percent of our caregivers had concerns: hardly anybody said they had no concerns.
There were a lot of worries about how young people would cope with the sight of blood, about practicalities of menstrual care: using products, managing personal hygiene, as well as how people would cope when their understanding perhaps lagged behind their physical maturity. For example, their body was changing, but would they understand why, and what was happening?
But then after menarche, once periods became more established, generally levels of concern about all of these things reduced. Still, about half of caregivers were worried about things like the practical aspects of menstrual care, and menstrual-related pain and communication about pain, as well as the impact of hormones on mood and behaviour.
A lot of these things were particularly concerns for caregivers supporting young people with higher support needs. There were also challenges around identifying pain when it’s presenting as behaviour. I am thinking about all of the other people working with our young people, and wondering if they realise that pain is being experienced.
Dr Liz Corcoran: That’s something we’ve seen echoed through other physical situations where behaviour that’s trying to communicate pain is then labelled as ‘challenging behaviour’ instead of investigated. That’s so important. Were there any findings that surprised you or changed your assumption about menstruation and Down syndrome?
Dr Katie Greenland: I didn’t really know what to expect. I was hearing so many different things. I just wanted to understand what the actual picture was. I think something that was quite surprising was that girls really were coping pretty well with the onset of periods. Many or most were just taking them in their stride, and that was something that was really surprising caregivers.
It was also really nice to see how many girls were pretty independent, especially those who had been menstruating for a number of years. One of the real reasons for this was the use of period underwear. This meant that girls could put on the underwear before going to school, and then often manage, or not even have to change the underwear during the school day.
I was also a little surprised about understanding and knowledge around the timing of onset of periods. Some people thought, ‘everything happens late with Down syndrome, they’ll get their periods later than their peers’. While others thought, ‘I’ve heard that people with Down syndrome start their periods really early’. Actually, what our survey showed was onset of periods was around age twelve, which is the same as the general population in the UK, and it’s similar to what other studies have shown as well. A lot of people just didn’t know this, so didn’t know when to expect that periods would start.
Dr Liz Corcoran: That’s really helpful. There’s a lot of mythology out there, and we now understand some answers to those things. Do menstruation experiences for girls with Down syndrome differ from those of other teenagers, particularly around communication, independence, or emotional well-being?
Dr Katie Greenland: I think one of the key differences is that more practical support is required, particularly in the beginning, with changing products and personal hygiene, and generally taking time to get used to products. Starting early sensitisation is helpful. There are some challenges around social appropriateness, and what was being communicated about periods more widely to the class or to wider family members. Generally, people were becoming reasonably independent as periods were establishing.
Less support was required than you might expect at school. While support was still required in many cases, many girls were able to manage residential trips without their parents there, while they were on their periods.
The key thing that we were seeing – as we find with Down syndrome – is a range of experiences. While a lot of people were not experiencing a huge number of challenges, nearly all the challenges were compounded for those with higher support needs. These are the young people who were struggling more with communicating when they’re in pain.
A lot of this stress was affecting the well-being of their caregivers and the whole family, with around a third of caregivers saying that they sometimes felt really overwhelmed about the practical support, and mental load, and everything else that came with just constantly thinking about managing what needed to be done, and thinking and worrying about whether their child was in pain, how much pain was being experienced, and whether they were able to effectively identify that and manage that.
Dr Liz Corcoran: And that was particularly seen in a subset: the more complex people with Down syndrome who have a dual diagnosis or other conditions going on. What practical advice then emerged from the study that could be immediately helpful for parents, caregivers, teachers, support workers? What can we say to them?
Dr Katie Greenland: One thing to say particularly for parents, is: don’t worry so much about it – although that’s easier said than done. It can be important even just knowing that for a lot of people, it is fine, with preparation. One caregiver said to us, that if she’d known there was even a possibility it would be okay (not a guarantee that ‘it would be fine’ because no one can say that), that would have helped lessen her worries before her daughter got her first period. In this instance, her daughter had quite limited communication, but still had really taken it in her stride.
Another thing, practically, that’s useful for people if they aren’t already aware, is using period pants. It’s helpful for people to know to investigate them. Some people said it could be a little complicated with dexterity issues, or in winter when you have lots of clothing: for example at school when you’re wearing tights, and trying to change period pants – that could get a bit complicated. A lot of people were using a pad inside period pants as well, so maybe the pad got removed, but the pants didn’t.
Other simple things include helping people orientate where the front of the period pants is: for example, sewing on a bow or some identifier that helps the young person be more independent, so they don’t put them on inside out.
Caregivers seem to be doing quite a lot of the other care aspects, like washing out period pants. Caregivers thought if they didn’t do that, then they wouldn’t be able to see how much blood came out, and therefore not know exactly how heavy a period was or be able to monitor it. Simple things can be done, like asking your young person to wash out their pants, but being there with them, so you can still see. It’s gradually increasing independence with little steps, based on the level that’s appropriate for the age and stage of the young person: giving them a little more independence bit by bit.
For teachers and support workers, again, it’s partly about realising how much people can do themselves. That’s a good start.
Dr Liz Corcoran: Yes, just like every other biological or life process: being a part of supporting that person to manage those changes appropriately, and scaffolding them with communication – everything that we’re already doing around life and growing up. That’s great. So, research is always really good at telling us where we need more research. Where did your research identify gaps in health services, or school support, or educational materials that we can give young people with Down syndrome?
Dr Katie Greenland: There are always gaps, and I think the point of identifying gaps is to know what needs to be done. Not always to say ‘we need more research to answer some questions’. Sometimes we do just identify gaps, and then we can start to fill them. In terms of healthcare, there did seem to be a bit of a gap in terms of guidance on decision making around use of hormonal medication. A lot of caregivers felt that they were sort of left to fend for themselves, in the sense that options were presented, but it was difficult to decide what to do, and they didn’t feel that there was enough support there.
I think that some resources and potentially training for clinicians would be useful, but perhaps resources also to help guide some of those decisions. It was quite a complex decision for people, since you’re taking a decision on behalf of somebody else. There’s a lot of ethics around this. People worry about whether it’s helping manage pain and symptoms of heavy periods perhaps in the short term, but what would the long-term health effects be? More information generally around hormonal medication would be really useful for people.
We interviewed some people in special schools, and also many of the young people that we interviewed were attending special schools. Generally, they seemed to be really good at providing support. They’re often used to helping support personal care. There was a gap in mainstream schools where if support was needed, the parent often needed to come into school and assist, for a number of reasons. I think perhaps there could be some more cross-talk between the school systems, to think more about that. At the moment there definitely seems to be a gap for girls with Down syndrome in mainstream schools.
In terms of educational materials: there’s definitely a lack of tailored materials for our young people. Some of this is not just the lack of the existence of materials, it’s a lack of dissemination of materials, and a lack of awareness of what is already out there. I think even within what’s already out there, there are still some additional areas where there could be more information, around some of these small steps towards supporting independence. People were really keen (young people and their caregivers) to know more about how to support independence, as well as seeking more information on hormonal medication, and practical menstrual care for both caregivers and young people.
Dr Liz Corcoran: How important do you think that early preparation is for menstruation education for girls with Down syndrome? Do we know yet what approaches work best when we want to prepare?
Dr Katie Greenland: I think we can learn a lot from the approaches being implemented in special schools, and from some of our specialist Down syndrome educators. Some efforts will need to be around translating these approaches into more mainstream settings.
It was interesting when we talked to people about their preparation, and talking at home about periods. For some people, that was difficult. It wasn’t a deliberate lack of preparation, but an inability to prepare for something that hadn’t happened yet. It’s a bit of an abstract concept for many of our young people, to understand something that they haven’t experienced. To some extent, preparing in that sense can be quite challenging. However people were still preparing by starting to sensitise around pads and panty liners, and getting young people to start wearing those so that they got used to them, as well as having open conversations and open-door type of policies at home so that the young people could watch their mother or maybe an older sister and understand a little more about what a period is.
Another thing that’s important – and perhaps was done better in special school settings – is beginning to give our young people some of the language that helps them talk about their emotions and pain, and the parts of the body that that pain is felt in. Not only in relation to menstruation, but simply thinking about body parts and emotions, and all those things that help facilitate communication about needs. Also we saw people using AAC devices to aid communication, but they didn’t have symbols for periods. Simply preparing by having the right symbols to be able to facilitate conversations would be really useful.
Dr Liz Corcoran: Giving people a vocabulary, so to speak, to communicate. Wonderful. What did our young women with Down syndrome themselves say? What did they want to tell adults and professionals – what did they want them to understand better, and what was their message to the world?
Dr Katie Greenland: A key thing is that ‘they can do it’. They were really keen to share experiences with younger people with Down syndrome, and let them know that it would be okay. They talked quite a bit about pain and pain management, saying things like: ‘when you’re in pain, you should think about the foods you like to eat, maybe take a heat pack and maybe rest a bit more and do the things you enjoy or watch television, relax’. A lot of what they wanted to share was about supporting people who don’t have their periods yet, which was really nice: and generally saying, ‘it’s okay’. They didn’t like their periods, but I think a lot of people don’t. I don’t think that’s entirely surprising. They also wanted people to understand that periods equaled pain, and that they found them yucky, and they didn’t enjoy having them.
Dr Liz Corcoran: It’s lovely to see that mentorship and sisterhood happening there as well in our community. Anything we can do to help dispel shame around this normal part of life is really important. From a funding perspective, why is research in this area so important? What wider social or health benefits could come from better support?
Dr Katie Greenland: Research is really important in this area because without it, we don’t know what people’s needs and challenges are. That lack of knowledge makes it challenging to make sure that people have the support that they need. If you haven’t done research to understand the range of experiences – not just what the challenges are, but who’s experiencing those challenges – then nothing can change, it will just be guesswork. I’d say research in this area has been really essential.
You ask what benefits and wider benefits could come. I think menstrual health – even in the definition of menstrual health – it’s not just about physical wellbeing, it’s about emotional wellbeing as well. Improving menstrual health can contribute to (as well as improved knowledge and confidence, being able to communicate needs, and understanding one’s body) improved independence, as well as emotional and physical wellbeing.
I think also it improves the wellbeing of caregivers too, because if our young people are better supported and become as independent as is possible for them, that relieves some of the burden on caregivers. While caregivers were very clear in saying this was part of their role, and they didn’t resent supporting at all, it was still taking a toll. The more that can be done to support families as well as young people, the better the mental health and wellbeing of our caregivers, which is therefore only good for our young people.
Dr Liz Corcoran: Absolutely. So, what are the next steps for this research? What kinds of partnerships or funding would help turn the findings into real-world support and resources?
Dr Katie Greenland: We do plan next steps. We’re not going to say that that ‘we’ve described the situation and that’s it’. You said earlier something about ‘researchers are very good at saying we need more research’. I’m going to say that, in one area, yes: I do think we need some more research, and that’s really around the presentation and communication of menstrual pain, and thinking a little bit more about pain and how we can understand what people are really experiencing.
And from different sides: helping people communicate their pain better, but also thinking about clinicians and others working with our young people, and how they can be better able to identify pain. Caregivers were using a lot of intuition and saying they sense from a change in behaviour, or by observing other aspects of their child, that they know that there’s pain there. For example: if their child loves dancing but they don’t want to dance, caregivers know that that’s linked to pain. I think we do need some more research on pain, and thought about how that research can be practically used in the interventions we would develop.
The other key thing to turn this into real-world support is developing intervention content. Sometimes this will be better dissemination of existing resources, and not reinventing the wheel. But also developing resources to fill some of the gaps that we have found in this research, and making tailored resources that are appropriate for different cognitive levels. For example: practical tools to aid independence and guide on menstrual care, communication about pain, hormonal options – some of the things we were talking about earlier – as well as some clinician training to encourage these holistic conversations about menstrual health. Perhaps also creating some supportive networks, and opportunities for peer-to-peer conversations to facilitate learning that way, too.
Whatever intervention that’s created would need to be piloted, and we would need to look at feasibility and acceptability of the content, to think about where and how interventions should be delivered, and then looking at how to scale up. I think there might be some partnerships possible with schools, thinking about what could be done in schools, and also in community organisations, and peer support, and how the two together could lead to an intervention that would improve menstrual health for our young people with Down syndrome.
Dr Liz Corcoran: Wonderful. At the heart of your research, as always, Katie, is the voice of the people who are affected or involved as well, which is great to see. Thank you so much for speaking with us and telling us about your work and what you’ve learned, and I can’t wait to see what comes next. As usual, thank you so much for working on improving the lives of people with Down syndrome – and best of luck for the future.
Dr Katie Greenland: Thank you for having me, Liz. We also want to let you know that we have a preprint of the research (available here). That’s the academic paper that describes all of our results in detail, and other aspects of the study. That’s available while we’re waiting for peer review in journal and publications.
Dr Liz Corcoran: Thank you, everyone, and have a lovely day.