Going To Hospital book breaks down barriers
The Foundation are proud to support a new book in the “Looking Up…” series that will improve access to healthcare for all people with LD, including those with Down’s syndrome. Released this week by Royal Cornwall Hospitals Trust and Cornwall Down’s Syndrome Support Group – CDSSG with the support of the Foundation, MENCAP and Inclusive Teaching Matters.
Going to Hospital breaks down barriers in the access to healthcare by making the journey to and through healthcare clear and simplified. Each page representing a step in the journey. The use of photos, words and Makaton symbols helps the reader to see what their trip will be like and take the fear and uncertainty out of an already stressful time.

This initiative is the work of co-authors Jane Rees from the NHS Learning Disability Nursing & Safeguarding Team at RCH Treliske and Angie Emrys-Jones Publications Lead of Cornwall Down’s Syndrome Support Group. Angie and Jane are passionate about supporting children & young people to be heard in the clinical setting by removing as many barriers as possible to make the hospital experience less intimidating or overwhelming to those with learning disability and or autism.
The booklet is easy read, uses Makaton symbols throughout to support images and is now available in hard copy which will be sent out to patients known to the Learning Disability Team at RCHT ahead of appointments or hospital admissions. Amanda Glennon of Inclusive Teaching Matters has produced a 10-page pdf of all the Makaton signs and symbols used in the book as Healthcare Prompt Cards which will be freely available to
both patients and staff on the Makaton Charity Website shortly. It is intended that wards use the download to provide now & next boards with a timeline of treatment – medicine/operation/sleep/wake up/eat/drink/toilet/home etc therefore creating a visual timetable for patients who need more support to embed their understanding and manage expectations of procedures or admissions etc

The Going To Hospital book is designed to be transferable to other trusts by enabling other hospitals to adapt and ‘tailor’ their own versions of the book and therefore being relatable in other areas of the UK. This will reach yet more people showing some of the procedures, equipment, and types of staff that children and young people with additional needs might see during their hospital visit.
The project has the support of Mencap’s national Treat Me Well campaign, the Downs Syndrome Research Foundation and also Paula McGowan’s #OliversCampaign following the preventable death of her son Oliver in 2016 due to poor care and inappropriate treatment. Oliver’s story, and others like his, are one of the main drivers for this project, we want to make sure the voices of our young people are heard in the clinical setting and that they are communicated with appropriately and are in control of their care as much as possible.

“It’s important that we are the healthiest we can be. This can sometimes mean that we need to go to hospital. Many people can feel frightened when they have to go to the hospital for lots of different reasons and that is perfectly normal. Lots of people find it difficult to explain exactly why they are so nervous. This fifth book in The Looking Up series is designed to help you to talk with your grown ups about why you are nervous and will help you to feel more confident to visit whichever department you need help from to be your healthiest self”
Paula McGowan, #Oliverscampaign
If you live in Cornwall and are not yet known to the Learning Disability Nursing Team at RCHT can request a copy directly for free and appointment letters will soon host a QR code of the book, meaning that it can be instantly downloaded directly onto a phone or device to be viewed at home.
Our Living Quilt
Every year at this time I find myself reflecting on what World Down Syndrome Day means to me that year. A culmination of what our resilient community has accomplish, changed and overcome as a whole. Whether it be a battle for disability rights being fought by a small group or many, it still boils down to the outcomes that affect us all. We may not agree on everything but one thing is for sure, our advocates are putting their heart and soul into each fight. We also know, the more unified we are in battle the stronger our voice will be.
That being said we know we certainly have room for growth in how we tackle our disagreements as does anyone with a difference of opinion. My hope this coming year is we are to be wise going forward and show respect and understanding for one anothers’ views when they differ and have healthy conversations with each other and hopefully understand one another better. Perhaps we cannot understand their point of view but
more often than not, everyone is coming from a position of love.
We ALL have so much to offer and bring to the table to improve the lives of our community. Medical experience (traditional and targeted), dietary advances and knowledge (food and supplements), educational knowledge, disability rights and various support groups all come to mind as some of the areas we can share and grow in. As we are a research foundation our charity is focused on getting promising studies funded and underway that can potentially become new ‘proven’ standard therapies that with allow everyone living with DS the ability to live their healthiest life.
Essentially when we stand back and look at our community from a distance, one that spans throughout time (past, present and future), we are a living quilt. Each sewn together with threads of love, steeped in the tears of events throughout our lives whether good or bad. A quilt often symbolises resourcefulness and moments in time. As we have spanned time, used what resources we have been afforded and been a collective covering for our community we too are all part of the patchwork of our living quilt. It is reflected in the faces, hopes or disappointment and the dreams of each child or adult on our quilt.  No patch is less valuable or needed than the other and each has impacted our lives either directly or indirectly teaching us where we need to grow and where we are succeeding, “We Decide”
No patch is less valuable or needed than the other and each has impacted our lives either directly or indirectly teaching us where we need to grow and where we are succeeding, “We Decide”
All of us at the Foundation wish all of you a Happy Down Syndrome Day 2020 and the very best this coming year. May we strengthen our love and support for one another as we reach for the stars for, and with all those living with DS.
Kindest Regards,

Human Rights: Woman with Down’s syndrome to challenge UK law
Heidi Crowter, a 24-year-old woman from Coventry who has Down’s syndrome, has joined forces with Cheryl Bilsborrow from Preston, whose two year-old son Hector has Down’s syndrome, and have launched a landmark case against the UK Government over the current discriminatory abortion law which allows abortion up to birth for Down’s syndrome.
Currently in England, Wales and Scotland, there is a general 24-week time limit for abortion, but if the baby has a disability, including Down’s syndrome, cleft lip and club foot, abortion is legal right up to birth.

There were 3,269 disability-selective abortions in 2018 and 618 of these were for Down’s syndrome. This represents a 42% increase in abortion for Down’s syndrome in the last ten years with figures rising from 436 in 2008. The figures are likely to be much higher – a 2013 review showed 886 foetuses were aborted for Down’s syndrome in England and Wales in 2010 but only 482 were reported in Department of Health records. The underreporting was confirmed by a 2014 Department of Health review.
The UN Committee on the Rights of Persons with Disabilities has consistently criticised countries which provide for abortion on the basis of disability.
The Committee on the Rights of Persons with Disabilities Concluding observations on the initial report of the United Kingdom of Great Britain and Northern Ireland made a key recommendation that the UK change its abortion law on disability so that it does not single out babies with disabilities. The Government has decided to ignore this recommendation.
The Disability Rights Commission (now the Equality and Human Rights Commission) have said that this aspect of the Abortion Act “is offensive to many people; it reinforces negative stereotypes of disability…[and] is incompatible with valuing disability and non-disability equally”.
The 2013 Parliamentary Inquiry into Abortion for Disability found the vast majority of those who gave evidence believed allowing abortion up to birth on the grounds of disability is discriminatory, contrary to the spirit of the Equality Act 2010 and that it affects wider public attitudes towards discrimination. The Inquiry recommended Parliament reviews the question of allowing abortion on the grounds of disability and should consider repealing section 1(1)(d) of the Abortion Act which allows for it.
Disabled peer Lord Shinkwin had a Bill in the House of Lords that would have repealed section 1(1)(d) of the Abortion Act – the Bill was undefeated but unfortunately ran out of time. Lord Shinkwin’s Bill was supported by Disability Rights UK.

Boris Johnson Government is currently deciding on the abortion framework that they will introduce to Northern Ireland ahead of March 31st. The proposed framework that the Northern Ireland Office has consulted on would allow abortion up to birth for disabilities including Down’s syndrome, cleft lip and club foot. 1875 people with Down’s syndrome and their families have signed a letter to Boris Johnson urging him to ensure that selective abortion for Down’s syndrome is not introduced to Northern Ireland.
Polling has shown that the majority of people in England, Wales and Scotland feel that disability should not be a grounds for abortion at all, with only one in three people thinking it is acceptable to ban abortion for gender or race but allow it for disability.
Heidi and her legal team have set up a CrowdJustice crowdfunding page to help raise the initial £20,000 to start legal proceedings, pay for legal advice and begin the preparation of the case. To find out more and to make a contribution to the case visit www.crowdjustice.com/case/downrightdiscrimination/
Heidi Crowter, from Coventry, who has Down’s syndrome said:
“At the moment in the UK, babies can be aborted right up to birth if they are considered to be “seriously handicapped”. They include me in that definition of being seriously handicapped – just because I have an extra chromosome! Can you believe that?
What it says to me is that my life just isn’t as valuable as others, and I don’t think that’s right. I think it’s downright discrimination!
The United Nations Committee on the Rights of Persons with Disabilities recently said that the United Kingdom should change its abortion law to make sure that people like me aren’t singled out because of our disabilities.
Sadly, the Government decided to ignore their recommendations and didn’t change the law. So now, I am going to take the Government to court with other members of the Down’s syndrome community to make sure that people aren’t treated differently because of their disabilities.”
Sally Phillips, actress and comedian, mother to Ollie who has Down’s syndrome told the Times:
“Given advances in medical care and quality of life for people with Down’s syndrome, the different right to life is beginning to look not just dated but barbaric.”
Paul Conrathe, the claimant’s solicitor from Sinclairslaw, said:
“This case addresses a matter that is fundamentally offensive and discriminatory- that unborn babies with a disability, and in this case Down’s syndrome, should be aborted up to birth. The current law reinforces negative stereotypes and attributes lesser value and dignity to people with disability.
In bringing this landmark case the claimants seek judicial ruling that the Abortion Act 1967 impermissibly violates the dignity of people with disabilities.“
Lynn Murray, spokesperson for Don’t Screen Us Out, said:
“By stating that disability is grounds for termination, section 1(1)(d) of the Abortion Act, promotes inequality. It would be totally condemned if a country’s abortion laws singled out babies on the ground of gender or skin colour, but because it’s a disability such as Down’s syndrome, that’s somehow ok? This is inequality, sanctioned, sponsored and funded by the state.
This provision in the Abortion Act is a hangover from a time when we had totally different attitudes to the inclusion and contribution of people with disabilities. You only have to look at the discriminatory language used by all sides of the debate in Parliament when this was discussed in 1967 and 1990 to realise how far attitudes have changed. Society has moved on but the law hasn’t. It’s time it did.”
We live in a society which proclaims that we want to empower those with disabilities, and that regardless of your background, you deserve a fair and equal chance at life. We believe that our laws must reflect this narrative.”
ENDS
reproduced with thanks to the Don’t Screen Us Out campaign
- For more information on the Don’t Screen Us Out campaign, see website www.dontscreenusout.org or email info@dontscreenusout.org
- For interviews, contact Don’t Screen Us Out spokesperson Lynn Murray on 0784 0966 736 or email info@dontscreenusout.org
- Heidi’s Facebook page:
- Previous news coverage featuring Heidi Crowter:
- https://www.theguardian.com/society/2018/dec/03/my-life-is-just-as-important-as-everybody-elses-meet-the-disability-leaders
- https://www.bbc.co.uk/news/av/45790521/the-23-year-old-busting-myths-about-down-s-syndrome
- https://www.itv.com/news/central/2019-03-21/he-makes-me-the-happiest-girl-in-the-world-twenty-three-year-old-with-downs-on-her-love-life-and-work-wouldntchangeathing-downs-syndrome-world-downs-syndrome-day/
- https://www.huffingtonpost.co.uk/entry/having-downs-syndrome-doesnt-make-me-less-of-a-person_uk
- https://www.dailymail.co.uk/video/news/video-1318649/Heidi-Crowter-s-powerful-s-Syndrome-message-Jeremy-Hunt.html
- Down’s syndrome abortion figures are expected to increase as NIPT is rolled out across hospitals on the NHS. The number of babies born with Down’s syndrome has dropped by 30% in NHS hospitals that have introduced the new test.
Non-Invasive Prenatal Test (NIPT) Fact Checking
Non-Invasive Prenatal Testing
by Colette Lloyd
Advertising is a dangerous thing. It can be used to inform people but also to mislead. We do need to know about someone’s product, but sometimes, in order to sell a product, advertisers go too far.
This happened in relation to non-invasive prenatal testing, and finally, in December 2019, followed by an enforcement notice in early 2020, the Advertising Standards Authority have recognised it. https://www.asa.org.uk/resource/enforcement-notice-nipt.html
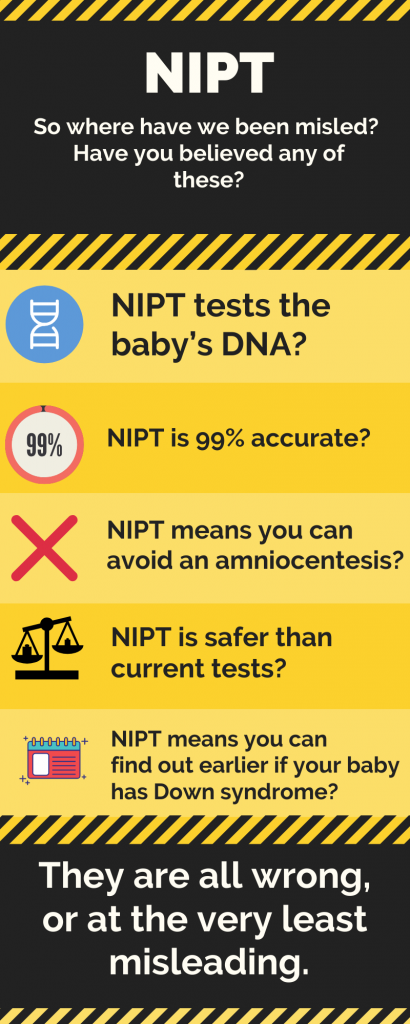
Dispelling the myths
Non-invasive prenatal testing uses fetal DNA, but fetal DNA does not translate to being the baby’s DNA. It is actually placental DNA that is tested. Why does this matter? Because the placental DNA can be different from the baby’s DNA, (although both are produced by fetal DNA), in a condition called placental mosaicism. This is one of the reasons that NIPT is unlikely to ever be 100% accurate. However, calling it the baby’s DNA makes NIPT seem more accurate than it is.
“It is actually placental DNA that is tested.”
Which brings me to accuracy. When a woman asks, “How accurate is the test”? what she is really asking is “How likely is it that my result will be correct?”. When a clinician asks it, they want to know “How many of all the babies with Down syndrome there are, will the test pick up?” Two very different questions. The answer to the second question is within the region of 97-99%. However the answer to the question women are actually asking is the Positive Predictive Value. And if you are in your 20s, the positive predictive value is as low as 46%. On a yes/no, 50:50 question. But those figures don’t sell tests. They might however, prevent a woman having unnecessary investigations during their pregnancy, or worse, an abortion based on misinformation. There is a calculator here for your PPV https://www.perinatalquality.org/Vendors/NSGC/NIPT/
 “And if you are in your 20s, the positive predictive value is as low as 46%.”
“And if you are in your 20s, the positive predictive value is as low as 46%.”
Therefore, considering these “accuracy” figures, you definitely can’t avoid an amniocentesis by having NIPT, unless you don’t really want to know for sure. In which case, you may want to ask yourself why you are having testing in the first place, unless you like to gamble. The test can be wrong both ways. It can tell you your baby does have Down syndrome when she/he doesn’t, and it can tell you your baby doesn’t have Down syndrome when she/he does. Therefore you do still have to have an amniocentesis to know for sure.
The safety statement is a red herring. It is safer than an amnio, but it doesn’t give you the same results as an amnio, so it isn’t really comparable. It is as safe as current screening tests which are also screening tests, just like NIPT.
And lastly to finding out earlier. Amniocentesis is safest when done after 15 weeks. There is another diagnostic test that can be done earlier called CVS, however, remember that placental DNA? CVS also tests placental DNA, so if NIPT is incorrect, CVS might be too. So you still have to wait for an amniocentesis to be sure. Sadly, not everyone has understood that, and the advertisers should be ashamed (The Journal.ie, 2019).
“…the advertisers should be ashamed”
For a copy of the leaflet for you or your healthcare professional click on the image below:

Recent News in Research
In 2006 the DSRF-UK held a research conference which included Professor Elizabeth Fisher from the Institute of Neurology, UCL who gave an excellent short summary and presentation on downs syndrome and the use of mouse models. Last week, a new study was released out of UCL, co authored by Prof Fisher, which is a great example of the insight and benefit of using mice models to gain more understanding in Downs syndrome.
Novel insight into chromosome 21 and its effect on Down syndrome
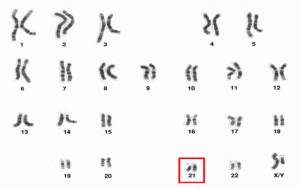
A UCL-led research team has, for the first time, identified specific regions of chromosome 21, which cause memory and decision-making problems in mice with Down syndrome, a finding that provides valuable new insight into the condition in humans.
Prenatal Screening and Down Syndrome – million-dollar ethics
Prenatal Screening and Down Syndrome – million-dollar ethics
The Nuffield Council on Bioethics, an independent think tank on bioethics, launched their report on the ethical issues of NIPT(non-invasive prenatal testing) in 2017. NIPT, a new more accurate way of screening for Down syndrome, is part of the genetic testing market, predicted to grow to a value of $22 billion by 2024.
NIPT raises many ethical difficulties, covered by Nuffield. However, the Down syndrome (DS) community did not agree with all of its conclusions. Sally Phillips, actor, comedian and mother of a young man with Down syndrome, made this clear in her response when she questioned the difference Nuffield had drawn between screening for sex and screening for Down syndrome. “For you we still fall the wrong side of the line… leaving DS in the significant medical conditions box you are saying that discrimination against their lives does not have the right to be protected against.”
However, the report did, at least, outline some of the issues to be resolved in order to have a more ethical roll-out of NIPT. Two years on, how far have we got?
NIPT is a groundbreaking technology that uses a sample of the mother’s blood, containing maternal and placental cells, to estimate the chance that the baby will have a genetic variation. It is already in wide use in the private sector, where companies in the UK are offering parents the chance to find out if their unborn baby has a higher chance of everything from Down syndrome to deafness.
PRENATAL CELL-FREE DNA SCREENING (CFDNA SCREENING) VIDEO (GENETIC SUPPORT FOUNDATION)
Some US companies are offering prenatal genetic testing to sequence the whole genome of babies, whilst others have suggested that we will be able to use genetic testing (not specifically NIPT) to identify the chance of the embryo having a low IQ. Further, a patent has been issued for using genetic testing to analyse unborn babies for the chance that they may have autism.
Back in the UK, the National Screening Committee announced their approval of the use of NIPT in the NHS screening pathway in October 2016, on a Saturday, in the Guardian, without waiting for Nuffield’s final report. However, although roll-out of free NIPT tests in the NHS was planned for October 2018, it is not yet officially part of the screening pathway. The hold-up was legal rather than ethical and that may soon be resolved. However, so far most of the ethical issues raised by the Nuffield report have not been addressed. I cover four main ones below:
- There continues to be no national care pathway for women wishing to continue their pregnancy following a high chance or positive result from testing (20, Nuffield Report). Neither NICE nor the Royal College of Obstetricians and Gynaecologists (RCOG) have prioritised this in the last two years. What little guidance there is remains buried in RCOG guidelines entitled Termination of Pregnancy for Fetal Abnormality published in 2010. Nuffield strongly suggested that the name of this guidance should be changed immediately to reflect the inclusion of continuation of pregnancy guidance and that that section should be substantially expanded, or separate guidelines should be produced.
- Misinformation continues to abound around what NIPT is and what it can do (6.8, Nuffield report). NIPT is a more accurate screening test, but it is not a replacement for a diagnostic test such as amniocentesis or CVS. Further, tests are evaluated by different measures, the difference between these appears to continue to elude manufacturers, clinics, midwives, consultants and the media. Sensitivity measures what percentage, of all tested fetuses that have the variant, the test will find. Positive predictive value of a result is how likely your high chance result is to have correctly identified the baby as having Down syndrome. NIPT will pick up 99% of babies in some populations, although the bias of available studies has been questioned by the Warwick systematic reviewers. However, if you are a pregnant woman, interested in how likely your high chance result from NIPT is to be correct, then the positive predictive values range widely, starting about 46%, depending on your age and combined screening test results. There is a useful calculator here.
- Nuffield also recommended that private companies be regulated, and their advertising controlled by the Committee for Advertising Practice (6.39, Nuffield report). There are now CQC inspections, but it isn’t making much difference to the misleading information being given in the advertisements.
- Genetic counsellors remain few and far between, and despite Nuffield highlighting this as a need, (6.30, 6.36, Nuffield Report) little has been done. Some courses to train already stretched midwives have been offered, but this has hardly plugged the gap. ARC( Antenatal Results and Choices) are offered as a solution. However, they haven’t collaborated with Down syndrome charities, as was suggested, And, although, the Nuffield report found them to be non-directive, the following facts call the usefulness of their helpline into question:
- they were formally known as SAFTA, (Support After Termination for Abnormality);
- they have received donations from manufacturers of NIPT totalling £11,500 from 2014-2017;
- their booklets strongly orientate towards the difficulties of continuing your pregnancy and they offer no support groups for women continuing their pregnancy.
What is needed is an NHS helpline staffed by trained genetic counsellors to help patients process all the prenatal genetic information that is now available. This has been called for by the Down Syndrome Association. The need was also clearly demonstrated, by a case in the press recently, where a woman was given a high chance result from a private clinic for Turner syndrome, with all the associated worry and suggestions of invasive testing only to realise, after much research, that her result was approximately only 40% likely to be correct.

The front cover of the new version of the leaflet
Some things have been done. For example, heads of screening in each NHS Trust have received training and Public Health England have revamped their Screening for You and Your Baby booklets and produced template letters for issuing test results. However, these are still not being used everywhere, with one woman recently receiving a letter saying “We are pleased to inform you that the blood test….. shows you are at low risk for Down’s syndrome’. What would they say to her friend whose child does have Down syndrome – commiserations?!
In this landscape it is very hard to see how women can make truly informed choices. And anyway, genetics do not tell you who your baby will grow up to be. They could be a famous actress like Sarah Gordy, or a Special Olympics swimmer like Shauna Hogan. They may marry the love of their life, like Maryanne and Tommy Pilling, have more complex needs that mean they need full time care, or like the majority, be somewhere in between. Everyone, including those with Down syndrome, are, thankfully, far more than their genetics.
Where does this leave us?
The NHS used to be for healthcare, but it is now far wider ranging than that. The technology is moving apace, and the UK is aiming to be at the forefront of the genetic revolution. We need to decide what place we will allow ethics to play in the face of this multi-million-dollar industry. And if we will allow ourselves to listen to the quieter minority voices of those whose communities are already being impacted.
Blog reproduced with thanks to CMF blog and to author Colette Lloyd who is a speech and language therapist and mother to a young adult with Down Syndrome