Dr Liam Fox MP introduces Down Syndrome Bill to Improve Life Outcomes
A Down Syndrome Bill is to be introduced to Westminster by Dr Liam Fox MP in the next Parliamentary session later this year. If successful, it will lead to the establishment of a Down Syndrome Act and a national strategy to improve provision and outcomes for all those living with Down syndrome in the UK. The Autism Act which became law in 2009 preceded the establishment of the national strategy to help meet the needs of adults with autistic spectrum conditions in England. The Down Syndrome Act will go further, identifying needs in all areas, for all individuals with Down syndrome across the whole of the UK. This will encompass, amongst other areas, maternity care, education, health, social care and employment.
The National Down Syndrome Policy Group, in coalition with the All-Party Parliamentary Group for Down Syndrome, has been lobbying for the long overdue Down Syndrome Act and have released a film featuring Founding Officers who have Down syndrome, highlighting some of the areas where they hope to see positive change in the future. Launch of The Down Syndrome Bill – YouTube
Dr Liam Fox MP, the Down Syndrome Bill Sponsor said,
“I am thrilled to bring forward a Bill to deal with the issues faced by those with Down syndrome. The full title is ‘A Bill to make provision about meeting the needs of persons with Down syndrome; to place a duty on local authorities to assess the likely social care needs of persons with Down syndrome and plan provision accordingly; and for connected purposes’.”
“My aim is to deal with three main areas. The first is to de-stigmatise Down syndrome and to re-educate both the public and professionals about the advances, including in life expectancy, that have occurred in recent decades. The second is to ensure that current provision of services is improved, whether provided by health, education or local services, by ensuring that providers give due consideration to those with Down syndrome when designing service provision. The third is to look ahead and deal with future issues, such as long-term care, in an era where, for the first time, many of those with Down syndrome will outlive their parents. By giving due thought to the issues today we can prevent avoidable human tragedies in the future.”
Actor and Founding Officer for the National Down Syndrome Policy Group (NDSPG) George Webster said:
“A Down Syndrome Act. Why didn’t we think of this before?!”
“We are all very excited that Dr Liam Fox is sponsoring a Bill with the aim of improving the lives of people living with Down syndrome.”
“I would like to see the Bill becoming law, then I think everyone like me with Down Syndrome will get better healthcare, more access to services and be more included in society. It is possible. It happens for some now, but it shouldn’t be a lottery. “
Peter Brackett, Chair of the NDSPG said:
“For too long the voice of the Down syndrome community has not been heard. We are delighted that the Down Syndrome Bill will enable engagement to secure and safeguard the rights and ambitions of the community across all aspects of society.”
“Having lobbied hard for this opportunity, our group will be fully behind Dr Liam Fox and the Down Syndrome Bill on its journey through Parliament, in line with our aim of raising the profile of issues affecting people with Down syndrome, their families and carers.”

Ends
- For more information, see the National Down Syndrome Policy Group website www.dspg.uk or email info@dspg.uk
- For media interviews with Dr Fox please contact David Goss David.goss@parliament.uk
- For interviews contact:-
-Ken & Rachael Ross MBE on 0771 0612 807 kenross@portsmouthdsa.org
-Lynn Murray on 0784 0966 736 or email lynn.murray@dspg.uk
-Peter Brackett on 0751 5121 733 peter.brackett@dspg.uk
- People with Down syndrome who are Founding Officers of the Down Syndrome Policy Group welcome the introduction of the Down Syndrome Bill: Launch of The Down Syndrome Bill – YouTube
- Line of Duty Star welcomes the launch of new APPG for Down syndrome https://www.heraldscotland.com/news/19295396.line-duty-star-tommy-jessop-backs-new-syndrome-all-party-parliamentary-group/
Line of Duty star with Down syndrome backs launch of new Down syndrome All-Party Parliamentary Group at Westminster
BBC’s Line of Duty star Tommy Jessop is backing the launch of the new All-Party Parliamentary Group (APPG) on Down Syndrome, which will be launched at an inaugural meeting at Westminster Wednesday 12th May 2021.

Actor Tommy Jessop, star of Line of Duty
A number of Down syndrome advocacy and support groups along with a cross-party group of MPs, led by SNP MP Dr Lisa Cameron and Labour MP Matt Western, have come together to launch the new All-Party Parliamentary Group on Down Syndrome.
The new group has been launched to raise issues affecting people with Down syndrome and their families and carers, as well as to promote equality and respect at all stages of life, to campaign for equal access and support in all areas of life and to highlight the innate worth of people with Down syndrome and the contribution they make.
The first meeting will include a speech by advocates with Down syndrome welcoming the establishment of the group and highlighting the issues that the group will be seeking positive change on. These issues range from maternity care for parents expecting a baby with Down syndrome to the matter of premature death for people living with Down syndrome.

APPG members will be supported by the newly-formed Down Syndrome Policy Group in the Secretariat role. The policy group is comprised of interest groups and individuals who have Down syndrome, therefore linking the parliamentary group to others with knowledge of the issues important to the wider Down syndrome community.
Line of Duty actor Tommy Jessop said:
“I welcome the new All-Party Parliamentary Group for Down Syndrome. I hope this will raise awareness of people living with Down syndrome and who we really are so that we really do have a voice to speak up for ourselves and other people”.
“I want to see people with Down syndrome treated equally with others before and after they are born. We are the only group of people in the UK where people try to end our lives before we are born just because we have Down syndrome. This is not fair. It scars our lives and causes mental health problems”.
Self-advocate Heidi Crowter, from Coventry, said:
“We hope that the members of the All-Party Group can use their powers and their energy to help make positive change for people like me and my husband James who has Down syndrome”.

Activist and Trustee of DSPG, Heidi Crowter
Conservative MP Elliot Coburn, the group co-chair, said:
“I was delighted to be asked to join the new All-Party Parliamentary Group on Down Syndrome, and to become a Vice Chair. People with Down Syndrome deserve a strong voice in Parliament to stand up for them and their families, and to press for greater support to help with the child’s development and for the family”.

Government Minister Caroline Dinenage said:
“I’m so delighted to support the All-Party Parliamentary Group for Down Syndrome. Portsmouth DSA is such a source of support, strength and positivity for so many individuals and families across our region. I am all in favour of action to ensure people with Down syndrome lead healthy, active and independent lives – that their talents are recognised and their voices heard”.
Warwick and Leamington MP Matt Western said: “The launch of this APPG is a chance for those in public life to celebrate the contribution of those with Down syndrome to their local communities, to the lives of their families and to British society in its entirety.
“It is vital we as politicians listen to those with Down syndrome so we can ensure that, through our work in Parliament, nothing holds people back from fulfilling their potential. I am proud to be part of this new APPG and I pledge to give those with Down syndrome a voice in politics whenever I can.”
Nicola Enoch from the Down Syndrome Policy Group said:
“We are striving to ensure that people with Down syndrome will have the opportunity to have their voices heard at Parliament. For too long their views have not been canvassed or heard; the APPG will provide a public platform for people with Down syndrome to speak”.

ENDS
-
For more information, see the Down Syndrome Policy Group website www.dspg.uk or email info@dspg.uk
-
For interviews, contact Lynn Murray on 0784 0966 736 or email info@dspg.uk
-
People with Down syndrome who are trustees of the Down Syndrome Policy Group introduce themselves: https://www.youtube.com/watch?
v=-zL0naw24a0&ab_channel= DownSyndromePolicyGroup -
Sharing the News Report 2019 – The maternity experience of parents of a baby with Down syndrome https://downsyndromeuk.co.uk/
flipbook.html -
Birth incidence, deaths and hospitalisations of children and young people with Down syndrome https://bmjopen.bmj.com/
content/10/4/e033770 -
Life expectancy and causes of death of people living with Down syndrome http://www.sldo.ac.uk/our-
research/life-expectancy-and- mortality/life-expectancy-and- causes-of-death-of-people- with-down-syndrome/ -
Down syndrome abortion figures are expected to increase as NIPT is rolled out across NHS hospitals. The number of babies born with Down’s syndrome has dropped by 30% in NHS hospitals that have introduced the new test. https://www.thetimes.co.uk/
article/new-test-brings-big- fall-in-birth-downs-babies- c89krkjcx
All Party Parliamentary Group (APPG) for Down syndrome
EXCITING ANNOUNCEMENT FOR OUR COMMUNITY
All Party Parliamentary Group (APPG) for Down syndrome being formed!
Over the past few years, a number of parent led organisations have been campaigning and lobbying in Parliament around issues, particularly in maternity care, that our community faces.
We discovered that there has not been an APPG for Down syndrome since 2015, so some of the groups have created an alliance to form an APPG. This will provide an opportunity for the views of people with Down syndrome and their families to be heard and addressed at Parliament. The APPG will give our community a platform to challenge some of the issues our families face and to raise awareness about living with Down syndrome in modern Britain.
An All Party Parliamentary Group (APPG) is a group of members from the House of Commons (Members of Parliament) and the House of Lords (Peers). It is all party because it has to have at least one member from the party in government (Conservative) and at least one from the main opposition party (Labour).
We have written to all Parliamentarians to invite them to join our APPG. It would be really powerful if as many people as possible could make contact with their local MP to request that they join our APPG on Down syndrome. Anybody who is allowed to vote can contact their MP and request they join – so we are asking people with Down syndrome to write and will be supplying an easy read version of this document together with a template. We hope that parents, siblings, grandparents, friends, professionals – anyone and everyone who is keen that the voices of people with Down syndrome are heard at Parliament will contact their MP.
We will be inviting people with Down syndrome to be involved with the APPG by participating in meetings and focus groups. If you have Down syndrome and are interested in being involved or have a family member with Down syndrome who is interested, please email dsappg@gmail.com
If you can add some of your own information in the first paragraph, it makes it more relevant and powerful. Please copy us into your email so we can record which MPs have been contacted. Email dsappg@gmail.com
APPG-For-Down-syndrome-easy-read
Dear (insert name of MP)
I am writing to you both as a member of your constituency and also proud parent/sibling/grandparent/teacher etc to (insert name) a (young person/child/adult) with Down syndrome. We would ask that you kindly consider joining the APPG for Down syndrome that is being formed to ensure the voices of those with Down syndrome including my (son/grandson/brother/student/friend etc) are heard at Parliament.
A coalition of national and regional groups have formed to act as the secretariat to the APPG.
The statement of purpose for the APPG is to campaign for equal access and provision to ensure equality and promote respect at all stages of life for people with Down syndrome.
Over recent years there have been huge advances in medical and educational development to enable people with Down syndrome to live full, rewarding and long lives, yet ironically whilst the future is looking so bright for our children and young people, outdated attitudes and legislation, discriminate against people with Down syndrome from the womb to the grave.
- In maternity services there is a blatant negative bias, with 69% of expectant women being offered a termination in the same conversation as being advised baby has Down syndrome.
- Termination to full term is permitted on the grounds of baby having Down syndrome. Women’s choices to continue are not supported with no care pathway and pressure to terminate – expectant women being told ‘it’s not too late’, at 36 weeks.
- In health care, the LeDeR report has cited that people with learning disabilities die on average 16 years younger than people without. It is estimated that 1,200 people with a learning disability die avoidably in the NHS each year.
- Employment opportunities are woefully inadequate, with only 6% of adults with a learning disability being in paid work.
- The annual research spending per person with Down syndrome to improve quality of life is currently in the region of £16.52, of which only £5.33 is towards treatment studies to test interventions.
People with Down syndrome deserve better and with your support we can ensure that their voices and views are represented to ensure equality for all.
I look forward to hearing favourably from you, should you require any further information please do not hesitate to contact me or the coalition by emailing dsappg@gmail.com
Yours sincerely
(insert your name)
NEW Pathway for Personalised Antenatal Care of Pregnancies Suspected or Diagnosed with Down’s Syndrome
Many within the Down syndrome community have for some time been concerned at the lack of a care pathway for those women expecting a baby with a high chance or confirmed result of having Down syndrome. Positive About Down Syndrome and the Downs Syndrome Research Foundation UK were invited to collaborate with St George’s University Hospitals, London to create such a document, which we are delighted has today been published.
The pathway is divided into six key areas:
- Antenatal Care – case-loaded by a named midwife or team for continuity of care
- Assessment for Fetal Structural Problems – to allow early care planning
- Assessment of the Risk of Prematurity -detection of polyhydramnios related to duodenal atresia
- Assessment of the Risk of Placental Dysfunction – detection of placental dysfunction will allow monitoring and timely scheduled birth
- Emotional and Psychological Support – use of unbiased language and attitudes and early access to psychological support (both formal and informal)
- Postnatal Considerations – opportunity to meet members of the neonatal team before the birth to discuss the postnatal plan of care
Dr Elizabeth Corcoran of the Foundation advises, “Absence of good practice pathways can mean poor and substandard care can flow into the gap. By leading the way with pathway we hope St George’s will be a beacon of antenatal care of women with pregnancies affected by Down syndrome.”
“We will ensure this pathway is shared to promote good practise and believe it will save lives.”
Nicola Enoch writes, “PADS provides online support to women with a high chance/confirmed result of baby having Down syndrome via DSUK PADS Great Expectations For Pregnant mums expecting LO w Down syndrome and it has concerned us how little support and information there is in some trusts around care of such pregnancies. We will ensure this pathway is shared to promote good practise and believe it will save lives.”
PADS and the Foundation thank St George’s University Hospitals NHS FT for acting upon the community’s concerns that pregnant women were not receiving care guided by the latest evidence or taking into account the poor care experiences.
We would ask that this pathway is shared to reach as many maternity units as possible.

Pathway document available here
REFERENCES USED IN PATHWAY
1. Muglu J et al. PLoS Med. 2019;16: e1002838.
2. Rasmussen SA et al. J Pediatr. 2006;148:806-812.
3. Skotko BG et al. Am J Med Genet A. 2009; 149:2361-7.
4. Sparks TN et al. Prenatal Diagn. 2016; 36:368-74.
5. Van Riper M and Choi H. Genetics in Medicine 2011; 13: 714 – 716.
Additional references of interest
Ivan, DL & Cromwell P.Clinical practice guidelines for management of children with Down syndrome: Part 1.Journal of Pediatric Health Care 2014; 28(1): 105 – 110.
Skotko BG, Capone GT, Kishnani PS; Down Syndrome Diagnosis Study Group. Postnatal diagnosis of Down syndrome: synthesis of the evidence on how best to deliver the news. Pediatrics. 2009;124(4).
Van Riper, M. A change of plans. American Journal of Nursing 2003; 103: 71 – 74.
Enoch N Sharing the News Report and UK Survey 2019
Phillips, C & Boyd, M. Relationship-based care for newborns with Down syndrome and endocardial cushion defect. Nursing for Women’s Health 2015; 19: 413 – 421.
Prenatal Care
#HoldsMeBack
“The only thing a prenatal diagnosis can provide is a first impression of who a child will be.”
A prenatal high chance or diagnosis of Down’s syndrome comes as just as big a shock to expectant parents as to parents who do not find out until birth. There are lots of conversations between parents as to which is the ‘easier’ way to find out.

A prenatal diagnosis means parents have had some time to process the news but they have lived with the worry of a higher chance of miscarriage and stillbirth(1). They have been asked, often several times to make ‘a choice’ and most likely overcome some negative and misplaced comments from the medical professionals looking after them. They have worried about how their child will be affected, what their needs will be, they have had sometimes difficult conversations with partners and probably had a few extra scans looking for ‘problems’. It was not an easy route but when baby arrives it is a time for celebration as parents finally get to meet their little one who has taken them on a different path to the one they expected at the beginning (2).
A postnatal diagnosis comes as a shock too, the longed for arrival isn’t as expected and no one quite knows what to say or how to respond. The tears flow even as a mother embraces her newborn, this is not what she wished for. These parents haven’t had months to adjust but have to rapidly catch up whilst caring for their new baby supported by maternity staff who may not know what to say or do. The consolation is they probably had a less stressful pregnancy, blissfully unaware of the adjustment they will have to make (3).

You’d imagine that one of the clear advantages of ‘knowing’ beforehand is that the maternity unit would be well prepared to support expectant parents and their little ones. You would think there would be a well researched pathway that all medical professionals could follow, making sure that these little ones are given the very best chance of arriving safely. You’d think there would at least be some national guidelines that identify what sonographers and consultants should be looking out for and what actions they should take. The sad fact is miscarriage and stillbirth rates are higher if the baby has Down’s syndrome but the sadder fact is that with better care and more supervision some of these deaths could have been prevented. We know babies with Down’s syndrome have a habit of arriving before their due date, we know the placenta might not be working as efficiently as it should and yet there is no clear plan as to how to manage these pregnancies to an successful outcome.
It is true a prenatal diagnosis doesn’t tell us of the full and love filled life that a child may have, the baby with Down’s Syndrome will write their own story just like any other child. But a prenatal diagnosis can have many advantages where care of mother and baby is research based and takes account of the possible complications, monitors appropriately and manages potential issues quickly should they arise. Sadly the Royal College of Obsteotricians and Gyneacologists has still not provided such a pathway despite much pressure from the Foundation and Positive About Down Syndrome. However we are proud to be working in collaboration with forward thinking practitioners who recognise the dangerous inconsistency in managing pregnancies where baby has Down’s syndrome.
You are probably not aware that just £16 per person with Down’s syndrome is designated for research (compared to over £200 per person with cancer). Of that paltry figure, £11 is spent on screening (4). The obsession with screening means improving the chances of wanted babies arriving safely is under researched and under funded. Please support the Foundation as we gather and commission research that helps inform and guide our health professionals.
——————————–
1 Sparks TN, Griffin E, Page J, Pilliod R, Shaffer BL, Caughey AB. Down syndrome: perinatal mortality risks with each additional week of expectant management. Prenat Diagn. 2016 Apr;36(4):368 – 74.
2 Skotko BG, Capone GT, Kishnani PS; Down Syndrome Diagnosis Study Group. Postnatal diagnosis of Down syndrome: synthesis of the evidence on how best to deliver the news. Pediatrics. 2009;124(4).
3 Van Riper, M. A change of plans. American Journal of Nursing 2003; 103: 71 – 74. & Enoch N Sharing the News Report and UK Survey 2019
Van Riper, M and Choi, H. Family-provider interactions surrounding the diagnosis of Down syndrome. Genetics in Medicine 2011; 13: 714 – 716.
Phillips, C & Boyd, M. Relationship-based care for newborns with Down syndrome and endocardial cushion defect. Nursing for Women’s Health 2015; 19: 413 – 421.
Non-Invasive Prenatal Test (NIPT) Fact Checking
Non-Invasive Prenatal Testing
by Colette Lloyd
Advertising is a dangerous thing. It can be used to inform people but also to mislead. We do need to know about someone’s product, but sometimes, in order to sell a product, advertisers go too far.
This happened in relation to non-invasive prenatal testing, and finally, in December 2019, followed by an enforcement notice in early 2020, the Advertising Standards Authority have recognised it. https://www.asa.org.uk/resource/enforcement-notice-nipt.html
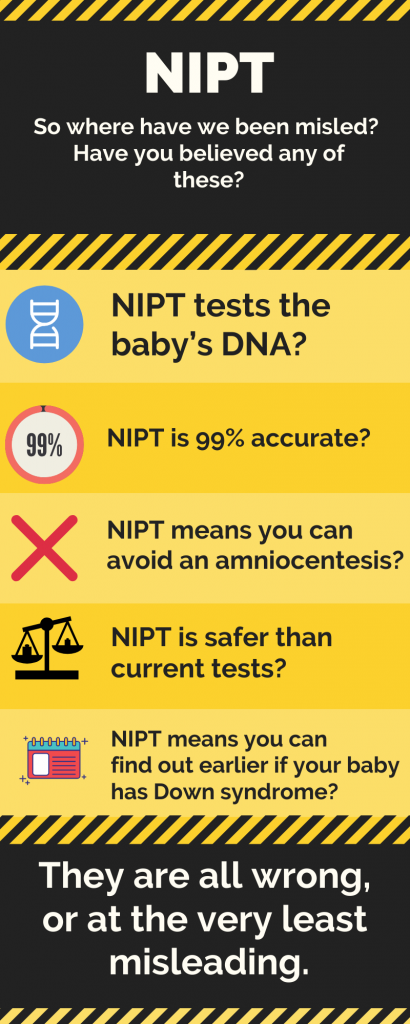
Dispelling the myths
Non-invasive prenatal testing uses fetal DNA, but fetal DNA does not translate to being the baby’s DNA. It is actually placental DNA that is tested. Why does this matter? Because the placental DNA can be different from the baby’s DNA, (although both are produced by fetal DNA), in a condition called placental mosaicism. This is one of the reasons that NIPT is unlikely to ever be 100% accurate. However, calling it the baby’s DNA makes NIPT seem more accurate than it is.
“It is actually placental DNA that is tested.”
Which brings me to accuracy. When a woman asks, “How accurate is the test”? what she is really asking is “How likely is it that my result will be correct?”. When a clinician asks it, they want to know “How many of all the babies with Down syndrome there are, will the test pick up?” Two very different questions. The answer to the second question is within the region of 97-99%. However the answer to the question women are actually asking is the Positive Predictive Value. And if you are in your 20s, the positive predictive value is as low as 46%. On a yes/no, 50:50 question. But those figures don’t sell tests. They might however, prevent a woman having unnecessary investigations during their pregnancy, or worse, an abortion based on misinformation. There is a calculator here for your PPV https://www.perinatalquality.org/Vendors/NSGC/NIPT/
 “And if you are in your 20s, the positive predictive value is as low as 46%.”
“And if you are in your 20s, the positive predictive value is as low as 46%.”
Therefore, considering these “accuracy” figures, you definitely can’t avoid an amniocentesis by having NIPT, unless you don’t really want to know for sure. In which case, you may want to ask yourself why you are having testing in the first place, unless you like to gamble. The test can be wrong both ways. It can tell you your baby does have Down syndrome when she/he doesn’t, and it can tell you your baby doesn’t have Down syndrome when she/he does. Therefore you do still have to have an amniocentesis to know for sure.
The safety statement is a red herring. It is safer than an amnio, but it doesn’t give you the same results as an amnio, so it isn’t really comparable. It is as safe as current screening tests which are also screening tests, just like NIPT.
And lastly to finding out earlier. Amniocentesis is safest when done after 15 weeks. There is another diagnostic test that can be done earlier called CVS, however, remember that placental DNA? CVS also tests placental DNA, so if NIPT is incorrect, CVS might be too. So you still have to wait for an amniocentesis to be sure. Sadly, not everyone has understood that, and the advertisers should be ashamed (The Journal.ie, 2019).
“…the advertisers should be ashamed”
For a copy of the leaflet for you or your healthcare professional click on the image below:

Sally Phillips’ address to the Royal College of Gynaecologists World Congress 2019
On Tuesday the 18th June the actress and mum Sally Phillips addressed thousands of doctors at the World Congress of the Royal College of Gynaecologists in London, England. Sally is well known in our community and beyond for highlighting the ethical issues around screening in her 2017 documentary “A World Without Down’s Syndrome” screened on the BBC. Since then Sally has continued to bravely speak out on the ethical issues around testing and the lived experience of a family that includes someone with Down’s syndrome.

Prof Basky and Sally Phillips at RCOG World Congress 2019 with Positive About Down’s Syndrome and Language Usage Posters
One doctor wrote to her and said:
Sally has kindly provided her speech to the Foundation to share the message far and wide beyond the professionals who could attend. We are deeply grateful for the bravery and passion with which Sally conveys the issues our community feel so strongly about. Thank you Sally!
Sally Phillips speech to RCOG World Congress 2019
“It’s been tremendously hard to work out what to say to you. The responsibility of representing my community, my friends and family to you in 10 minutes has been almost overwhelming.
WE WANT TO TALK TO YOU
Once they knew I had been invited 5 parents sent me scripts fully, written. I’ve been inundated with quotes, statistics, slides, baby photos, wedding invites, play fliers, school reports, certificates of achievements. It’s made me feel a little inadequate. Olly’s best primary school certificate was for ‘most enthusiastic bouncer’.
I’ve been sent articles by educators and LD nurses detailing how different the medical model is from the real people they encounter in their work. I’ve been sent leaflets made by mothers in their spare time, posters, paid for by Mums for you to put up in hospitals, articles they’ve written, drafts of charters for proper antenatal care for mothers with known pregnancy of DS that they work on late at night, unpaid, when the kids are asleep. On top of this, once again my inbox and all my social media streams are jammed with women’s testimonies of traumatising encounters with doctors, midwives and counsellors on receipt of a prenatal diagnosis.

Sally Phillips address the RCOG 2019 World Congress
How to tell our stories and be heard? Not as a box ticking exercise but actually heard and absorbed, not listened to and then dismissed as emotional, or biased, or unhelpful, but taken seriously. Being taken seriously is a problem for me generally. But this time it really matters. As you can see, I’ve decided to come camouflaged as an artist’s impression of the inside of my womb in the hope that this will make you more receptive.
We know that you are good people who do great work in difficult circumstances, we know you didn’t go into medicine to cause harm, but in my ten minutes, on behalf of my community I am here to tell you that intentionally or not, harm is being done to us. Whilst NIPT and associated tests represent a technological advance they do not yet represent a genuine improvement in caring for women during pregnancy.
ETHICS
Ethics and Unforeseen consequences of NIPT is our title today. Quite late to be thinking about the ethics? The ethics often seen like an add on to us – a post-hoc justification – an ah shit did I turn the taps off thought – carried out while clearing away the champagne glasses and party balloons from the launch of the latest technological breakthroughs in Down syndrome detection. This, for the record, feels to us, families living happily with Down Syndrome (I’m not lying about that) – in tremendously bad taste.
DROP IN BIRTHS UNFORSEEN?
And do we or don’t we discuss the drop in Down syndrome births after the introduction of NIPT, because it’s pretty hard to argue that that was unforseen. In fact, comments were made during the review process that indicated that a drop in the birth rate, ethical or not, is still viewed by some here as one of the benefits of NIPT.
We were told that although both conception and termination rates would rise considerably the actual birth rate would remain the same. Like the Down syndrome population was to be managed, like a group of pandas, or endangered toads (depending on your attitude to disability) or something.
Was that ethically acceptable reasoning? I don’t know, I’m not an ethicist. I’m a sitcom actress. But as parent. It turned my stomach,
What has happened in reality? Well, Public Health England don’t know because they’re not monitoring it because It’s complicated, apparently. NIPT is offered differently in different hospitals and not the same offer as FASP are recommending and besides they’re busy, they haven’t got round to it yet.
Colette Lloyd, a friend of mine, a Mum, a speech and language therapist writes “They’re supposed to be evaluating the rollout, how can they evaluate if they are not monitoring it? It’s a disgrace that the NHS doesn’t care enough about our population to be bothered with doing this- it’s a continuation of the issues highlighted by Panorama and the LeDer report (3 people with a learning disability die avoidable deaths every day in NHS care) It is their responsibility happening on their turf, following endorsement of a product by them”.
So Colette, being a dynamic sort of person, taught herself statistics and she has spent weekends and evenings for over year now poring over freedom of information requests to local hospitals. She has four children and a job by the way.
Her figures are doing their second round with the National Office of Statistics (correction: statisticians) and will be launched on the Today programme in the near future. No doubt to be met with the usual universal indifference. Sneak preview – in those hospitals which offer NIPT the DS live birth rate is down 30%, in those hospitals that do not offer NIPT it is down 9%.
Why is this important to us? It’s a vicious cycle. A reduced birth rate has a knock-on impact. Reduction of friends, reduction of investment in research to improve quality of life for those with Down Syndrome, reduced incentive to provide appropriate schooling, work opportunities, means increased isolation for our population, increased poverty and therefore separation from the rest of us. People fear the unknown. People with Down syndrome not being known in turn means more terminations.
We knew this was going to happen. You knew it was going to happen. The manufacturers knew it was going to happen. We are in pain in my community because put simply, everybody knew it was going to happen and nobody could care less. What attitude towards our population does that betray and how does this attitude impact the way you talk about Down syndrome to pregnant women, who are, although, yes, strong and yes trustworthy, also vulnerable, desperate to do the best for their child and suggestible.
But it’s women’s choice I can hear you cry! It’s informed consent! None of us in this room would want to be called eugenic. There is a grim history of coercive societal policies to improve the health of the population, we know it’s wrong now. That’s why the focus now quite rightly is on ‘informed consent’, and reproductive autonomy, people making their own individual decisions. But since screening was created for many reasons, none of them the empowerment of women, I think the women’s choice rationale often sits uncomfortably on its’ public health and eugenic foundations and the welcome scrutiny it has come under through introduction of NIPT has revealed some areas where choice is not truly the priority.
Why is the Downs test a screen and not a test? Why do we have a law that allows abortion for severe handicap without defining what that handicap is? If Down syndrome is discovered, as I believe it will be, to be always mosaic in nature, is informed consent ever possible as the unknowables are so huge.
If individual decisions now are made within a system and in a context which is biased and overwhelmingly carries them towards certain outcomes then the end result is the same as if you had coerced them in the first place.
I am here as a repository of stories from my community. Tom says ‘anecdotes are not data’ – I say ‘anecdotes are just stories which are not data yet’. When we present women with a screen and not a one off test, when it becomes so routine it’s opt out not opt in, when pregnant women, who yes are adults and trustworthy, but who as must be admitted are also vulnerable and suggestible are repeatedly questioned, repeatedly told that the only reason other women do not terminate is because they are too scared to, when they are told not to speak to people with lived experience of Down Syndrome because they overstate the positives, when they are told there is no support or help for them continuing a pregnancy, when they are made to feel guilty for bringing a baby to birth, then this constitutes a biased context. I agree with Jane that making women carry a baby they do not want to is appalling. I happen to think that pressurising them into terminating a wanted baby is possibly worse.
Many women are repeatedly offered terminations even after expressly saying they did not want them. I ask you on their behalves – has the fear of ‘wrongful birth’ lawsuits altered practice? Has this anxiety spread from you to your work and your patients that people feel they have to offer terminations again and again.
I had this yesterday from a woman whose daughter is two:
“I’m starting an online support group for women who have been left with mental health problems as a result of being offered terminations against their wishes repeatedly. Being forced to imagine killing your own child is so completely unnatural. It’s like the fear and grief of knowing your child was in imminent danger of dying/being murdered but mixed with the sick feeling of you being responsible. Even the counsellors are struggling to know how to help us. Mine is using a strategy she uses to recover soldiers from PTSD.”
Can I ask you. If our mothers were considering legal action would that change your practice?
We all have prejudices we aren’t aware of that might not look so bad at first glance. I’m more concerned when people think they aren’t prejudiced. When Olly was born I was told ‘he’s very loving and he’ll love music’. This is the same thing well-meaning people said about Jamaican immigrants in the 50’s.
It is impossible to hide 100% how you feel about disabilities and saying every time ARE YOU SURE is a dead giveaway that you think women continuing are making the wrong decision.
Nuffield quite rightly recommended that a pathway be established to support women who choose to continue their pregnancy. You’ve had two years to do this and while advocates and supporters of women who help women through termination have managed to get you to fine tune car for them, nothing has yet been done to create a support pathway.
I challenge you to shore up the erosion of choice that exists for women carrying an affected fetus with DS. Lay a strong foundation for both choices. Don’t let the women who continue fall off a cliff due a lack of robust clinical guidelines. Don’t assume a lack of these guidelines means society thinks she TOOK A WRONG TURN and you need to ask, maybe for the 2nd maybe the 10th time “are you lost dear?”
Second. NIPT is driven by the industry. The industry are trying to sell their product. They are good at this. They need high numbers to undergo screening to turn a profit. The global NIPT industry is expected to be worth over $6 billion dollars by 2025. These are serious players. They are not care providers. They are not to be messed with. When I made my documentary I got a lot of online trolling from all corners, but the worst came from city traders. “Now get out the fucking way”.
Even the name ‘Non-Invasive’ is a marketing tool as it is not currently diagnostic and the positive predictive value of the test in a younger woman, in the absence of other screens is – correct me Basky – around 48%. The dangers of amnio have been massively overstated – Professor Nicolaides told me that he lost 1:1000 healthy babies after amnio, Lyn Chitty that her rate was 1:600. But the manufacturer literature puts this rate as 1:100.
By this time most of the major players in this field have benefitted from industry funding. If you all have taken money and benefits does that make it ok? Not to us, the ‘canaries in the mine’ to use a term for the DS community first coined by Tom Shakespeare.
If making money out of testing that leads in most cases to selective termination is not a form of eugenics, I do not know what is!
Be on your guard against spin. Companies have long recognised that using trusted individuals is an effective way to promote their products. David Cameron is a lobbyist for Illumina. I hope they’re regretting that. Even support groups are now getting funded by business, so they become advocates for NIPT. In the States manufacturers have set up their own support group where counsellors funded by them give online support to families and then train them up to talk about their (always positive) experiences of NIPT to medics. Some of our parents have been flown out to the States to be taught how to advocate for better information in pregnancy via NIPT. This practice of cultivating fake grass roots support for a product is known as astroturfing and has been supercharged by the internet. We have seen neutral parent speakers replaced with manufacturer vetted parent speakers at medical events. A parent who severed her ties with Illumina last minute was replaced.
It is also being noted by various practitioners of medical ethics – Professor Becki Bennett and Panagiota Nakou, for example, at the University of Manchester, that elements of spin, that over-represent positives about the test are creeping into titles, introductions and conclusions of scientific research papers. Not the research, not the methodology, but the way it is presented. I read their response to a paper which had been published in the Journal of Medical Ethics, a paper which was supported by the Wellcome Trust. Be sure of what you are reading and hearing. I’m just going to say two words. Brexit and Trump.
By this point, you will be saying: but it’s still women’s choice, it’s not coercion. Three things.
First, the information is often not either balanced or the information women need– it may give you data about the test, but it does not give good information about the real lives of people with DS and other disabilities.
We tell you over and over that we are happy with our family members but we are not believed. I could show you Brian Skotko’s paper, a survey of 2000 families that says that 98 percent of people with Down syndrome are happy with their lives, 97 percent love their family member, but the respondents were selected from families in support groups so some argue the study was skewed. Perhaps it’s better to challenge you to show me a single paper that demonstrated that people with Down syndrome and their families were not happy.
Second, the health professionals may be biased.
Not because they are bad people. But because we are all biased to some degree.
Third, the context of screening is a conveyor belt. I think the word is ‘path dependency’. We don’t have enough genetic counsellors and specialist midwives. Providing a test implies that people should have the test. People who decline the test are asked again and again, to the point of trauma, why they have not had it.
Evidence shows that people adapt to disability. But it takes time. When you have a spinal injury or contract MS, you may want to die. You may think your life is over. But all the empirical evidence shows that you adapt, you change your environment, you come to terms, and life goes on, just as happy as before. Tom has data for this. Marcia Van Riper’s study of over 3000 parents from more than 50 countries showed that while 25% saw Down syndrome as a tragedy on diagnosis, given time only 0.68% felt the same way.
And this is a central issue with NIPT that I haven’t heard discussed. That our stories often involve that devastation at diagnosis which often comes about through lack of knowledge and changes pretty fast leaving parents with huge feelings of guilt for having been so upset to start with. Because it’s so efficient, with NIPT prospective parents do not have time to adapt. The vast majority of people who carry on with pregnancies have good outcomes. But many others end pregnancies, thinking they are doing the best for their families, and not knowing of the joy that families and people with DS experience.
Finally, we talk about the benefits, but we don’t talk about the harms that result from screening. The anxiety for all pregnant women. The distress at terminating wanted pregnancies. The distress for people with DS and other conditions who feel very unhappy that society is sending the message that they are not wanted. The way that a shrinking population may find it harder to get medical expertise, educational expertise and the other supports that they need to lead good lives.
Is it enough, we ask, for a population group to be targeted for screening because another more powerful or more numerous population group has a gut feeling that their lives are crap. Is that enough? We don’t think so.
My personal belief is that if we allow unrestricted freedoms here, a consumerist ethic at this point, that we end up with an increasingly unfree society. Where the median becomes increasingly homogenous, ideas of normality become increasingly restrictive and conditions conceived of as unliveable with become more and more numerous.
You, rightly or wrongly, to some degree hold the future of our community in your hands. Please take more care as you move forward.”
Prenatal Screening and Down Syndrome – million-dollar ethics
Prenatal Screening and Down Syndrome – million-dollar ethics
The Nuffield Council on Bioethics, an independent think tank on bioethics, launched their report on the ethical issues of NIPT(non-invasive prenatal testing) in 2017. NIPT, a new more accurate way of screening for Down syndrome, is part of the genetic testing market, predicted to grow to a value of $22 billion by 2024.
NIPT raises many ethical difficulties, covered by Nuffield. However, the Down syndrome (DS) community did not agree with all of its conclusions. Sally Phillips, actor, comedian and mother of a young man with Down syndrome, made this clear in her response when she questioned the difference Nuffield had drawn between screening for sex and screening for Down syndrome. “For you we still fall the wrong side of the line… leaving DS in the significant medical conditions box you are saying that discrimination against their lives does not have the right to be protected against.”
However, the report did, at least, outline some of the issues to be resolved in order to have a more ethical roll-out of NIPT. Two years on, how far have we got?
NIPT is a groundbreaking technology that uses a sample of the mother’s blood, containing maternal and placental cells, to estimate the chance that the baby will have a genetic variation. It is already in wide use in the private sector, where companies in the UK are offering parents the chance to find out if their unborn baby has a higher chance of everything from Down syndrome to deafness.
PRENATAL CELL-FREE DNA SCREENING (CFDNA SCREENING) VIDEO (GENETIC SUPPORT FOUNDATION)
Some US companies are offering prenatal genetic testing to sequence the whole genome of babies, whilst others have suggested that we will be able to use genetic testing (not specifically NIPT) to identify the chance of the embryo having a low IQ. Further, a patent has been issued for using genetic testing to analyse unborn babies for the chance that they may have autism.
Back in the UK, the National Screening Committee announced their approval of the use of NIPT in the NHS screening pathway in October 2016, on a Saturday, in the Guardian, without waiting for Nuffield’s final report. However, although roll-out of free NIPT tests in the NHS was planned for October 2018, it is not yet officially part of the screening pathway. The hold-up was legal rather than ethical and that may soon be resolved. However, so far most of the ethical issues raised by the Nuffield report have not been addressed. I cover four main ones below:
- There continues to be no national care pathway for women wishing to continue their pregnancy following a high chance or positive result from testing (20, Nuffield Report). Neither NICE nor the Royal College of Obstetricians and Gynaecologists (RCOG) have prioritised this in the last two years. What little guidance there is remains buried in RCOG guidelines entitled Termination of Pregnancy for Fetal Abnormality published in 2010. Nuffield strongly suggested that the name of this guidance should be changed immediately to reflect the inclusion of continuation of pregnancy guidance and that that section should be substantially expanded, or separate guidelines should be produced.
- Misinformation continues to abound around what NIPT is and what it can do (6.8, Nuffield report). NIPT is a more accurate screening test, but it is not a replacement for a diagnostic test such as amniocentesis or CVS. Further, tests are evaluated by different measures, the difference between these appears to continue to elude manufacturers, clinics, midwives, consultants and the media. Sensitivity measures what percentage, of all tested fetuses that have the variant, the test will find. Positive predictive value of a result is how likely your high chance result is to have correctly identified the baby as having Down syndrome. NIPT will pick up 99% of babies in some populations, although the bias of available studies has been questioned by the Warwick systematic reviewers. However, if you are a pregnant woman, interested in how likely your high chance result from NIPT is to be correct, then the positive predictive values range widely, starting about 46%, depending on your age and combined screening test results. There is a useful calculator here.
- Nuffield also recommended that private companies be regulated, and their advertising controlled by the Committee for Advertising Practice (6.39, Nuffield report). There are now CQC inspections, but it isn’t making much difference to the misleading information being given in the advertisements.
- Genetic counsellors remain few and far between, and despite Nuffield highlighting this as a need, (6.30, 6.36, Nuffield Report) little has been done. Some courses to train already stretched midwives have been offered, but this has hardly plugged the gap. ARC( Antenatal Results and Choices) are offered as a solution. However, they haven’t collaborated with Down syndrome charities, as was suggested, And, although, the Nuffield report found them to be non-directive, the following facts call the usefulness of their helpline into question:
- they were formally known as SAFTA, (Support After Termination for Abnormality);
- they have received donations from manufacturers of NIPT totalling £11,500 from 2014-2017;
- their booklets strongly orientate towards the difficulties of continuing your pregnancy and they offer no support groups for women continuing their pregnancy.
What is needed is an NHS helpline staffed by trained genetic counsellors to help patients process all the prenatal genetic information that is now available. This has been called for by the Down Syndrome Association. The need was also clearly demonstrated, by a case in the press recently, where a woman was given a high chance result from a private clinic for Turner syndrome, with all the associated worry and suggestions of invasive testing only to realise, after much research, that her result was approximately only 40% likely to be correct.

The front cover of the new version of the leaflet
Some things have been done. For example, heads of screening in each NHS Trust have received training and Public Health England have revamped their Screening for You and Your Baby booklets and produced template letters for issuing test results. However, these are still not being used everywhere, with one woman recently receiving a letter saying “We are pleased to inform you that the blood test….. shows you are at low risk for Down’s syndrome’. What would they say to her friend whose child does have Down syndrome – commiserations?!
In this landscape it is very hard to see how women can make truly informed choices. And anyway, genetics do not tell you who your baby will grow up to be. They could be a famous actress like Sarah Gordy, or a Special Olympics swimmer like Shauna Hogan. They may marry the love of their life, like Maryanne and Tommy Pilling, have more complex needs that mean they need full time care, or like the majority, be somewhere in between. Everyone, including those with Down syndrome, are, thankfully, far more than their genetics.
Where does this leave us?
The NHS used to be for healthcare, but it is now far wider ranging than that. The technology is moving apace, and the UK is aiming to be at the forefront of the genetic revolution. We need to decide what place we will allow ethics to play in the face of this multi-million-dollar industry. And if we will allow ourselves to listen to the quieter minority voices of those whose communities are already being impacted.
Blog reproduced with thanks to CMF blog and to author Colette Lloyd who is a speech and language therapist and mother to a young adult with Down Syndrome