Concerns about the McArthur Assisted Dying Bill in Scotland in relation to Down’s Syndrome
The Down’s Syndrome Research Foundation UK recently sought the opinion of people in Scotland about the currently debated McArthur Bill on Assisted Dying, regarding issues with consent and coercion in relation to people with Down syndrome. The McArthur Bill in Scotland would legalise assisted dying for terminally ill adults over the age of 16 who meet the required criteria. The legislation is in the final stage of the Scottish Parliamentary process, and MSPs are currently debating amendments to the Bill. The final vote by MSPs is scheduled for Tuesday 16th March 2026.
Polling was carried out by independent body Whitestone Insight. The majority of people who participated in the polling expressed concerns. Some highlights of the polling include:
Three-quarters (75%) of Scots said they were concerned that it would be difficult to establish whether a person with a learning disability, such as Down’s Syndrome, would be expressing voluntary informed consent if they applied for assisted suicide. Only 14% reported being unconcerned.
Two-thirds (67%) of Scots said that a person with a learning disability, such as Down’s Syndrome, might be particularly vulnerable to the risk of coercion or manipulation into an assisted suicide if it became legal. Only 20% disagreed.
Dr Elizabeth Corcoran from the Down’s Syndrome Research Foundation UK says:
“This polling shows Scots are deeply concerned about the negative impact that legalising assisted suicide will have on people with intellectual disabilities, such as Down’s syndrome.
We are deeply concerned about the risks of coercion and undue influence in relation to the proposed change to the law. In particular, people with Down’s syndrome and people with intellectual disabilities in general are at significant risk of coercion and undue influence, in part due to their need to trust and build understanding for their needs with caregivers and medical professionals.
There is a very real risk that, if passed, this legislation could be applied far beyond its original intention. It may be stretched to include people who are not at the end of life, but who are instead viewed as having lives that are devalued through discriminatory attitudes and narratives. For our community, that possibility is terrifying.
This concern is not hypothetical. The committee examining the proposed legislation has recognised that the bill may be challenged under the European Convention on Human Rights, resulting in eligibility being widened. Should that occur, there is every chance that eligibility could be widened. No one, not this Parliament, nor any future one, can guarantee how such laws will be interpreted or expanded over time.
Disabled people in Scotland already struggle to access the care and support they need, with nearly three-quarters of respondents to a recent Inclusion Scotland survey stating they had “problems accessing services from their local council”. Rather than legalising assisted suicide, a more appropriate use of scant public resources would be to redouble efforts in Scotland to remove barriers to care.
We are calling on MSPs to ensure our community is protected and vote against the McArthur Bill at Stage 3.”
DSRF UK is concerned that, as with Kim Leadbeater’s Assisted Dying Bill, the human rights and needs of people with Down syndrome have not been fully considered, and the risks that the Down syndrome community faces in relation to assisted dying legislation is not widely understood.
We urge you to contact your MSPs in this crucial moment as they consider their vote.
The Ongoing Impact of Covid Lockdowns on Children with Down Syndrome: new report
A new report from University College London has just been published, examining the effects of Covid lockdowns on young children with Trisomy 21. Children with Down Syndrome in Lockdown: Key findings from a survey of parents of children under 11 with Down Syndrome in the UK
It’s clear that deeply challenging consequences were set in motion by the pandemic lockdowns, and this negative course has not yet been corrected. This report comes at a key time while the draft statutory guidance for the Down Syndrome Act is still currently under consultation. Meeting the need for integrated provision of services is an aim directly addressed by the Down Syndrome Act: this report is a perfect example of why this matters, and a particularly acute instance of ways that children with Down syndrome are affected when services are fragmented or suspended.
Report Findings: interconnected impacts on wellbeing
The report presents findings from a UK survey of 241 parents of children aged 0–11 with
Down syndrome, examining the impact of COVID-19 lockdowns on education, health, development, and family life. Families reported widespread disruption, with interconnected effects across multiple areas of children’s wellbeing.
Education was heavily affected. Although most children attended school pre-pandemic, 91% stopped in-person attendance during the first lockdown, and fewer than half attended during the second. Remote learning was often ineffective: many children struggled to engage online, only about half received remote provision, and parents frequently had to manage learning themselves. Most parents believed their children missed key learning activities and worried about long-term academic regression. Extracurricular activities also largely stopped.
Social and communication development declined for many children. Nearly 60% of parents reported deterioration in social skills, and over half noted changes in communication ability, often attributed to reduced social contact and limited therapy support. Some children became more anxious or cautious around others.
Mental health and behaviour showed notable deterioration. About two-thirds of parents reported negative emotional impacts, with increases in unhappiness, anxiety, tantrums, defiance, and aggression. Isolation, disrupted routines, and fear related to COVID-19 were key contributors.
Daily life impacts were mixed but meaningful. Sleep patterns were mostly stable, but over half of children experienced reduced physical activity. Diet changes were variable, with some increases in sugary and processed foods. Many families faced financial strain, employment changes, and increased caregiving pressures.
Health services and support access were significantly disrupted. Around 90% experienced cancelled or delayed medical appointments, and many therapy services stopped or moved online. Parents feared these gaps contributed to stagnation or regression in development.
The report concludes that children with Down syndrome experienced substantial, interconnected harms during lockdowns. It calls for integrated, family-centred support, targeted educational catch-up, improved access to services, and further research into long-term impacts.
Recommendations included these observations: “… investing in early intervention and preventative initiatives can prevent future health and wellbeing challenges across the life course. Making sure that support is sufficiently available across health, education and development could not only improve quality of life of people with DS in the short term, but could have lifelong individual, societal and economic benefits, including the reduction in future demand for health and support services. As part of the government’s reassessment of how their policies can be more disability-inclusive, we suggest that working with families to develop and invest in tailored, evidence-based and sustainable solutions that acknowledge the impacts of the pandemic could help to mitigate any damage caused by the lack of support families experienced.”
The report’s findings will be of great importance in finding the best way forward for some of the young people who still remain worst affected by the pandemic. We also hope that its findings will shed light on why we have campaigned so hard for the Down Syndrome Act 2022 and for effective guidance. We hope to see a fractured system being looked at more holistically, for the sake of the DS community who are often harmed in a lasting way by the omissions and gaps they encounter. With thanks to the team at UCL for their insightful attention to the impact of the lockdowns on young children in the DS community.
International Workshop (Potenza, Italy)
Therapeutic Perspectives for Intellectual Disability in Down Syndrome
Date: Saturday 18 April 2026
Location: Auditorium, Ospedale Regionale San Carlo, Potenza (Italy)
Under the patronage of: Regione Basilicata
Organised by: AIPD Potenza and the Italian T21 Task Force
DSRF-UK is pleased to share details of an international one-day workshop bringing together clinicians, researchers, and families to discuss emerging therapeutic approaches to intellectual disability in Down syndrome. The programme spans disease mechanisms, translational science, and clinical trials, and ends with an interactive public roundtable designed to connect the science with the lived experience of families. (The organisers are also offering online participation—registration details below.)
Provisional programme (18 April 2026)
Morning — Institutional opening & Scientific Session 1
08:30 Registration
09:00 Welcome and institutional greetings
09:30–13:00 Morning scientific session
Chairs: Filippo Caraci (Catania), Vittoria Infantino (Potenza), Angelo Carfi (Rome)
09:30–10:15 — Laura Cancedda (Genoa, Italy)
Restoring neuronal chloride homeostasis to treat brain disorders.
10:15–11:00 — Rafael de la Torre (Barcelona, Spain)
AEF0217 and endocannabinoid receptor modulation: translating synaptic mechanisms into cognitive benefits in Down syndrome.
11:00–11:30 Coffee break
11:30–12:15 — Joaquin M. Espinosa (Aurora, USA)
Clinical trials for immune modulation in Down syndrome.
12:15–13:00 General discussion & Q&A
13:00–14:00 Light lunch
Afternoon — Scientific Session 2 & Roundtable
14:00–17:30 Afternoon session
Chairs: Eugenio Barone (Rome), Antonella Izzo (Naples), Emanuela Abiusi (Rome)
14:00–14:45 — Laurent Meijer (Roscoff, France)
Phase 1 clinical trial of Leucettinib-21 (a DYRK1A kinase inhibitor) targeting Down syndrome, Alzheimer’s disease, and Parkinson’s disease.
14:45–15:30 — Nelly Pitteloud (Lausanne, Switzerland)
GnRH as a potential therapy for Down syndrome.
15:30–15:45 Coffee break
15:45–16:30 — Isabel Barroeta (Barcelona, Spain)
Clinical trials for Alzheimer’s disease in Down syndrome: progress, challenges, and perspectives.
16:30–17:30 Interactive roundtable with public, speakers & families
Open dialogue between science and community.
17:30 Closing remarks
A few speaker highlights (what they’ll be covering)
- Translational neuroscience (Laura Cancedda): focusing on how neuronal “balance” mechanisms (like chloride homeostasis) may be relevant to brain function and treatable pathways.
- Synapses and signalling targets (Rafael de la Torre): presenting work on endocannabinoid receptor modulation and how synaptic insights might translate into measurable cognitive benefit.
- Immune modulation and trials (Joaquin M. Espinosa): looking at immune pathways in people with Down syndrome and what it takes to run rigorous clinical trials in this space.
- Targeting DYRK1A (Laurent Meijer): an update on early-stage (Phase 1) clinical evaluation of a DYRK1A inhibitor—an area of strong interest because DYRK1A is implicated in issues faced by people with Down syndrome.
- Hormonal pathways (Nelly Pitteloud): discussing GnRH as a potential therapeutic avenue and what the evidence is pointing to.
- Down syndrome and Alzheimer’s trials (Isabel Barroeta): a practical overview of where the field is now, what’s hard about trials in this population, and what’s coming next.
Registration (and online access details)
The flyer directs registration via the link below (the organisers can share participation/online-connection details after sign-up):
Register here

Legacy Giving: ‘Remember a Charity’ Week is 8th to 14th September 2025
This week, we’ll be putting legacy giving in the spotlight. ‘Remember A Charity’ Week is a great opportunity to think about the charitable work you support, and the causes you want others to know more about.
We would love if you would consider supporting the Down’s Syndrome Research Foundation UK, as gifts like this make a huge difference to the Foundation and allow us to continue our work.
For ideas on practical steps you can take, we have put together some information that you may find helpful. Another great resource, giving answers to Frequently Asked Questions on leaving a gifts in your will, can also be found here.
We are linking with Remember a Charity to promote this way of supporting charities. They have some excellent practical tools:
- You can write your will for free online using their partner’s services.
- Further, we can also share a benefit available to our supporters in this week: you can register your will for free this week at the National Wills Register using the code: RACWeek2025. Registering your will helps safeguard your final wishes.
You can also read some inspiring stories of people who have helped us in the past.
Together, we can truly achieve remarkable things (like launching the world’s first Down Syndrome and Sleep Research Network) – and we cannot do this kind of work without your support. Leaving us a gift in your will truly makes a difference.
Thank you for your help, in every way, big and small.

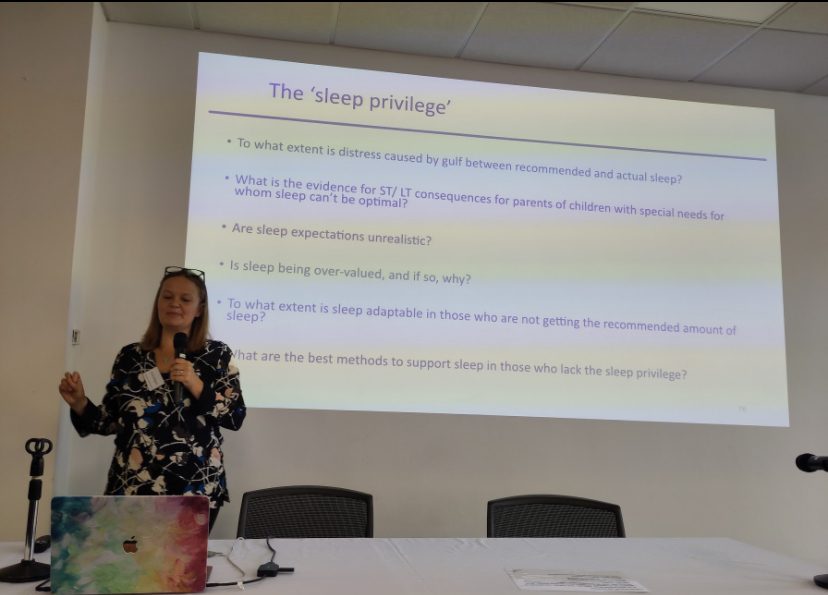
Adaptability of sleep and the ‘sleep privilege’: the need for new research
How much should parents and caregivers worry about sub-optimal sleep? This issue was recently brought to our attention by Professor Alice M Gregory, a keynote speaker at the recently launched Down Syndrome and Sleep Research Network (DSSRN).
Sleep issues are over-represented and under-researched in the Down syndrome community. This gap is a driving motive for the DSSRN, and through this new research network, we hope to accelerate knowledge and effective interventions in this area.
The effect of broken sleep often weighs on parents and carers. This includes the health impact of poor sleep on family members with Down syndrome, but also the consequences of long-term interrupted sleep on caregivers themselves.
Prof Gregory has been involved in research with particular interest for caregivers. Her presentation at the DSSRN launch, “Type 1 diabetes as a prototypical condition challenging what we know about sleep”, opened up very interesting considerations about the pitfalls of an exaggerated focus and concern about quantifying and qualifying sleep.
Sleep is certainly more important for health and development than we have realised historically, but there are adaptive patterns that are even less understood, which may help compensate for some quantifiable sleep deficits.
This ability to adapt is also an under-researched area. Exploring this further will bring solid evidence that can help shape practice and guidance. This may be very good news for many people who simply cannot secure the ‘sleep privileges’ that others enjoy, and may ease some of the worries that come along with poor sleep.
We believe that this topic is just one of many areas that will benefit from the support of the DSSRN, bringing researchers together to change what we know about sleep in the DS community.
For further details on this topic, you can read a newly published editorial in the Journal for Child Psychology and Psychiatry, by Professor Alice Gregory et al, “Sleep privilege – research and clinical recommendations for when sleep cannot be optimal”.
Assisted Dying Bill Updates
Last Stages involving MPs
We now have a quick email tool available to use to contact your MP, asking them to cast their final vote against Kim Leadbeater’s Assisted Dying Bill. As we have mentioned in previous blogs, we consider that this piece of legislation will change the whole landscape of care in a way that will detrimentally affect people with Down syndrome, as well as many other people.
This Friday, MPs will gather in Westminster, preparing to vote for or against the Assisted Dying Bill for the last time. After this, if the Bill progresses, the chance to stop assisted dying passes out of MPs hands.
It’s a critical time to reach out and let your MP know that you have urgent and serious concerns, and do not want them to vote in favour of the Bill. The upcoming date is:
Friday 20th June 2025: Final Commons Vote at the Third Reading
- The elected members of parliament who represent us will decide if they will let the Bill pass, and then responsibility to stop it or move it onwards passes over to the House of Lords.
- On this day your MP will vote for the final time on whether Assisted Dying will become legal in the UK.
Some important things to remember:
- MPs Daniel Francis and Sarah Olney who served on the Bill Committee have spoken out strongly at the recent Report Stage proceedings in Westminster, about how the Bill will affect people with intellectual disabilities – they claim that legitimate concerns are unaddressed and the Bill is unsafe for people with disabilities of any sort
- All proposed amendments to the Bill that would have safeguarded people with intellectual disabilities, including those with Down syndrome, were voted down by the majority pro-euthanasia Bill Committee
- Many major concerns have repeatedly emerged, with some MPs declaring openly that they will switch sides due to their concerns
- The vote looks like it will be very tight because of shifting opinion – and that’s why your communications to your MP could truly make a difference, even at the last minute
You can find the email tool here – it takes only seconds to send a letter to your MP. Thank you for all your efforts on this profoundly important issue.
“You shouldn’t be dying just because someone else has deemed you unworthy.”
DSRF was privileged to speak recently with Jen, who has an eye-opening perspective on the Assisted Dying Bill, as a healthcare professional and a mother in the DS community. As we approach the final vote for MPs on Friday 20th June, Jen’s story is a must-read. Please share this story with anyone who has not yet realised the wider context that Assisted Dying will fit into, and how this change in the healthcare climate will affect people with DS.
I’m Jen, mother of D. who is 24 years old and has Down syndrome, and we are from Northwest England. I have been feeling moved to speak out recently to warn people about the dangers of the Assisted Dying Bill. I don’t think people have a clue how dangerous it is to introduce this as a law.
What is your background?
I am qualified as a Registered General Nurse, and worked as an advocate for children with disabilities for short time. I have worked as a family group conference coordinator to support families to develop a plan to prevent children going into care. I was also involved as a lay assessor when the Quality Outcomes Framework for GPs was introduced with regards to accessibility. I have worked in adult social care as a Care Coordinator / Assessment Support Officer. I am also a ‘Partners in Policy Making’ parent, and trained by a family rights group – they gave me an eye-opening training course, about personalisation, choice and control.
I am now retired. First and foremost, I’d describe myself as D.’s Mum – she is my raison d’etre and greatest joy.
With all the professional experience I have gathered over the years, I know how things work from the inside, and that’s why I can’t ignore the dangers and the attitudes that I know will shape the direction this Bill will take in practice. Back when I did nursing, we used to refer to people as ‘the hysterectomy in bed 5’: we’ve moved on and learned a lot more since then, but the dehumanisation definitely still exists, and I’m constantly on the watch for it.
Once we start with assisted dying, rates of use will go up and the system will get away with it, like they are doing in care homes already with DNARs (Do Not Attempt Resuscitation orders). Working in adult social care, I saw with my own eyes how blanket orders of DNAR were given out, to people with dementia and to other vulnerable groups. During Covid, a disproportionate number of people with intellectual disabilities died. There are so many reasons why I am worried about the Assisted Dying Bill, and it’s all from what I have experienced and been through.
I’m quite feisty and well equipped to fight for our rights, but I’ve seen that when some people get into a crisis in a hospital, they get ‘white coat syndrome’ and assume that the doctors always know best. However, the doctors don’t know your child. They may have training as a doctor but there is still a lot they need to know. There’s always a context that only the carer knows in depth, and unfortunately the habit of ‘othering’ the patient is very harmful and affects the kind of care they get.
What alarms you about the Assisted Dying Bill being proposed in the UK?
I think right now we’re on a timeline that isn’t progressing anymore but going backwards for people with Down syndrome. In the 1980s a lot of breakthroughs happened, and kids with Down syndrome were deemed educable, and moved out of institutions and back into the community, and life improved for many. However often the infrastructure to support these changes wasn’t there, and ground workers were often set up to fail. Now I think we’re seeing cost cutting measures, with money concerns really being put to the forefront. I am really convinced that Assisted Dying is all about money at the very bottom of the issue.
I am always guarded about things that are set up as shiny and all about doing good, because I’ve found that there can be darkness behind it. It’s a bit like family planning: it has origins in the eugenics movement. I am seeing a lot of comments from people online about who should qualify for an assisted death, describing some people as a drain, and having no value – but how do you measure value? You shouldn’t be dying just because someone else has deemed you unworthy: that’s my great concern. It’s really important for society to learn how to care and empathise, and how to slow down, because aging and death are part of life for everyone.
What do you think about general attitudes concerning people with Down syndrome?
There is a constant fight that happens around D. It’s nothing to do with her: my daughter has taught me so much and is an absolute joy. It’s a fight with society, to say she is worthy of having an ordinary life, worthy to enjoy a normal life.
This battle starts at the moment of conception: this is not just about assisted dying. About 98% of women who find out they are pregnant with a child who has Down syndrome have an abortion nowadays. You can’t tell me that 98% represents an informed choice on this. There’s a huge amount of fear and pressure put on women, and a lot of the time that’s why they terminate. It’s a really frightening slippery slope to force women on. There are incidents that are horrific and I have never been in those situations. I am so glad, however, that I didn’t have a test that would have told me D. had Down syndrome before she was born. I had a wonderful pregnancy with no pressure and I never had to justify why I wanted my child to live. I was living in Holland then, and didn’t experience any pressure there at the time, but here in the UK now it’s all medicalised. I am so glad I didn’t have to go through all that process and could just sail through my pregnancy. In the end, it’s such an unknown – you can’t really plan. Everyone thinks differently but I didn’t feel like dreams or aspirations were wrecked – I was just waiting to see the baby that was in my tummy, and it was D.
The night D. was born and the midwife told me she had Down syndrome, I held her and thought “maybe it’s just you and me now, little one, because dad might find this too much”. For me the oxytocin was rushing in and I was totally in love, but I was worried about how my husband would cope. I kept giving the baby to him all the time, and by day three he was in love too. I was wondering, ‘will she ever do this? will she ever do that?’. Now I laugh when I think about how ill-informed I was, but so many wrong things are told to mums and it’s all the information they have. Reactions of staff are often terrible, and those first reactions can inform your initial bonding with your child. One doctor asked my friend at her child’s birth: “have you noticed something about your child? He has a face you might have to grow to love.” These attitudes are not coming from the parent but show the bias of the healthcare professionals.
I’m not saying it’s easy, but we have no guarantees in life, and being a mum isn’t easy anyway. I think about my friends who are mums of teenagers: they have some different concerns than I do, but we all have concerns!
Please tell us about the challenges you have encountered in trying to get adequate care for your daughter.
I’ve seen a lot of twisting of the rules to suit what organisations want to do. For instance during lockdown when people could still go to school, I got a phone call saying that D. ‘couldn’t’ go to college: they just applied a recommendation without discussion with her or us, and made it seem like a rule. Blanket bans on people like D. being able to access college were a form of ‘othering’ and discrimination, and they were applied at unnecessary times.
D is definitely the ‘comeback kid’ – she has been through a lot and come back every time. Some things were missed when she was a baby and mistakes were made in her care. Her hips have been dislocated since she was a child, and she is now in a wheelchair. This has put strain on her heart and she gets tired really easily. It all stems from what was missed when she was a baby.
She had a Ventricular Septal Defect (VSD) surgery to repair her heart at the age of 14 months, and there were unnecessary post-operational complications, caused by a push to get beds cleared on the unit to make way for the next day’s operation list. This resulted in her having to be put on life support, on a Cardiac ECMO (Extracorporeal Membrane Oxygenation). It was the catalyst for a horrific set of events. We had to bring our young child home tube-fed, she had an extremely diffuse EEG after prolonged resuscitations, she lost all muscle tone and had to have a double ileostomy as a result of a perforated bowel from sepsis. Often we say she is like Lazarus – she has really beaten the odds to be with us still.
Some recent incidents have also been traumatic due to the way we were treated. During lockdown she went into sudden onset cardiac arrest in the early hours of the morning. Thankfully I heard her and went running in to work on her. The paramedics arrived and got her to hospital, and the very first thing the A&E consultant asked is, ‘what is her quality of life?’. She asked me this at 3 o’clock in the morning in the middle of the hospital corridor. I went nose-to-nose with her and said, ‘Don’t you dare ask me that, you would never ask this question if she didn’t have Down syndrome. Get back in the room and save her life, do what your Hippocratic oath asks of you!’
I have a lot of contacts now in healthcare, and thankfully we were granted access to D. even when she was ventilated, and I worked hard to make her humanity evident to people. I put up photos of her everywhere, and I spoke to all the staff who knew her. I was with her all the time and calmed her down when she was extubated by being there, and they allowed me to be there as part of the team. I asked them to treat her just like any other 21 year old – something that definitely didn’t happen when we were in A&E.
Everyone who meets D. loves her, but I always have to prove her worth before they meet her. Unfortunately when people see things on paper, they make biased assumptions. I had to fight to get a defibrillator implanted, and only one place was willing to fit it: after the fact they said it was the right thing to do, but it only happens after a lot of discussion and effort to humanise her to professionals.
As I get older, I think a lot like that MP Daniel Francis who spoke at the debate in Westminster recently, who asked ‘what happens when I am not there?’. He too has a daughter with a learning disability and knows this law won’t have the safeguards that are needed. I am like a lioness on her behalf, but I won’t always be there.
Does the healthcare profession value your insights or help you in ways you need?
I think professionals are most often doing what they can to help, but the bigger frame they have to fit into often doesn’t seem to value life.
It’s helpful when we are able to respect each other’s expertise, and we need each other. At this point, our GP office knows I won’t waste their time, and that I have never been proved wrong when I have a concern. They will see D. that day if I ask for it. D. can present as aclinical, but she could be in renal failure, and I know how to spot signs they can’t see. I know when she is ‘off’ simply because I know her so well.
The problem is that you can never afford to take your foot off the pedal, and without other people helping, it gets harder as you get older. Resilience is my best and worst trait. I am well informed and well educated on these issues, and sometimes that leads to people thinking you’ll get on and do it, and even do their job for them.
I asked for some support from the local hospice for advance care planning, as D. is life-limited. When it comes to my own daughter, what I can do for someone else actually can’t be done by me. I need a witness and support. I know that the Learning Disability nurses are over-stretched, but it was really disappointing that they simply posted paperwork for advance care planning through my door and left me to it. No matter how capable I am, I am still a mum who has feelings: this is my daughter and I can’t fill out paperwork like that on my own.
What do you think about the likelihood of coercion and mental capacity issues in relation to this Bill?
The communication needs of people with Down syndrome are absolutely not understood – professionals cannot get their heads around capacity and are still wrangling with the mental capacity act.
When D. was in hospital a few years ago, the charge nurse breezed in in the morning, and said “so a mental capacity assessment has been done on D. …”, and I stopped her right there and asked, ‘When??’ I was there with her all the time, and I didn’t see any mental capacity assessment being done. I was told that it was done at 3am – when we were both asleep!! Even if they had woken her, how can you carry out an accurate mental capacity assessment on someone who has been woken up in the middle of the night? That is a falsification of a document – I asked the nurse if she was simply keeping her KPIs up, and told her that this was disgraceful.
Unfortunately these kinds of bad practices already happen! They will probably introduce quotas for how many people they need to help die, and the majority of people will be totally unaware of it. They introduced the fragility scale during Covid and didn’t tell people about it, so many were forced into things they didn’t know was a possibility.
My big concern is that admin staff are just looking at numbers, and that doesn’t translate into the worth of a life.
I am really concerned about the coercion issue. My daughter is always saying ‘sorry mum, my brain is mush’, and it’s because she is tired – I reassure her and I know how to help her understand. However, when she got to the age of 18, suddenly professionals won’t discuss things with parents in the same way, and you need to go through the Court of Protection to get the right to be consulted – but who has the money to go through all that?
I am also appalled about the fact that amendments to the Bill to protect people with intellectual disabilities weren’t approved. The whole Bill is being rushed and rushed, and isn’t getting the publicity and scrutiny it needs. It isn’t Love Island, so it isn’t hitting the headlines, but we’ll all be affected by this in a much bigger way than people realise.
When people get older and tired they look to professionals for guidance and advice, and these same professionals are stretched and pressured and may have biases that they are not aware of. They may make decisions that will have horrific consequences.
They say that the Bill has strong protections like needing two doctors who agree, but DNARs also needed that, and look how that turned out. Who will vet these doctors and make sure they aren’t Dr Kevorkians? Doctors already aren’t trained in many things they need to know. I think it’s a horrific scenario.
How do you keep a positive outlook among all these serious issues?
I think in the end, death is part of life. It’s really important to focus on dying a natural dignified death, not prematurely ending life because the person doesn’t feel seen or valued. It’s possible to live and die really well even with pain, illness, age and disability. However, I always say to my husband, don’t ever pull the plug on me, because you know I will be fighting to get back! Valuing life like this has always been innate to me. I have seen families who have kids with many different conditions, and they adore and value their children’s lives. People who are on the outside don’t know the person and their value. Cost will never come into it with me – there is enough money in the world. In the 80’s we were going in a better direction than now – right now everything is commodified.
I wish I could bottle up all the love and joy I have from my daughter. She is just herself. She doesn’t often ask about how having DS makes her different – and to me, she is just my daughter. Sometimes she notices that some things aren’t fair, but I encourage her and remind her that it’s like that for everyone in some way.
There are some wonderful things we’ve been able to do recently. We were on holiday in Menorca and were delighted by the accessible beaches that could be reached by beach wheelchairs. It made me think when I came back home, we are by the ‘leisure peninsula’ of England and yet no-one with a wheelchair can access our own beaches. A friend in an organisation called ‘Make It Happen’ put me in contact with a local councilor who was able to draw down funding from the local authority and the NHS to realise this dream, and we got beach wheelchairs that people can use free of charge, with one dedicated to my daughter. She is definitely the catalyst for helping others and making their needs evident, it’s her legacy to help others access the simple pleasures that are denied to them.
Seeing my daughter’s joy every day helps me through everything and gives me the motivation to fight everything that comes in my path that is a threat to her. Right now, the new threat on the horizon is definitely Assisted Dying, and I want other parents to wake up to where this could lead.

Email or call your MP if you have any doubts https://members.parliament.uk/FindYourMP
World’s first research network focused on sleep issues and Down syndrome launched
Researchers from institutions across the UK gathered in London to foster cooperation in tackling sleep disorders that can profoundly affect health and development in the Down syndrome community.
The Down Syndrome and Sleep Research Network (DSSRN) was officially launched on Monday at the conference hall of the National Council for Voluntary Organisations, as an initiative to bring scientists together to concentrate on one of the highest priorities and most promising focal points for improving quality of life for people with Trisomy 21.
Sleep issues are common in people with DS, being detected up to ten times more than in typically developing peers. Researchers are keen to explore how improvements in sleep could positively impact development, cognition, chronic illnesses, and also longevity in a population whose life expectancy is at least 20 years lower than average.
Presenters included academics and researchers from University of Cambridge, Kingston University, Royal Holloway, Great Ormond Street and other institutions, presenting on their individual work and setbacks they have faced as researchers. A panel discussion with five interdisciplinary researchers generated a lively conversation on the challenges and opportunities in this area.
The role of sleep dysfunction in Down syndrome Alzheimer’s disease: Novel applied methodologies Dr Stephanie S. G. Brown Ph.D. – Senior Research Associate and Alzheimer’s Research UK Fellow, Department of Psychiatry, University of Cambridge
Keynote speaker Dr Lizzie Hill (Senior Lecturer in Sleep Physiology, University of the West of England (UWE Bristol) said “All of us in this room have heard something to the effect that ‘people with Down syndrome don’t sleep well’ or ‘it’s just part of the condition’, but that doesn’t mean we shouldn’t investigate and treat these as we would for anyone else.”
A poll of attendees on the day showed that 55% of attendees were currently involved in research, and 45% planning / would like to get involved, but experiencing barriers including lack of funding, lack of time and high workload, lack of research skills and knowledge, lack of support, bureaucracy and admin issues, ethics and regulatory processes, difficulty finding collaborators. Many of these issues were addressed on the day to explore ways forward.

Prof Cathy Hill- BM MSc PhD FRCPCH – Professor of Paediatric Sleep Medicine – Southampton University
The DSSRN has secured funding for its startup year with generous grants from Hospital Saturday Fund, the Baily Thomas Charitable Trust, and the Sir Samuel Scott of Yews Trust, and the Launch Event was sponsored by Inspire Medical Systems and Idorsia. The DSSRN’s founding and launch have been coordinated by the Down Syndrome Research Foundation UK (DSRF UK), a charity promoting and funding medical research to improve the lives of people with Down syndrome since 1996.
DSRF UK’s Chair Dr. Elizabeth Corcoran said: “It has been a dream to bring these highly renowned researchers together to begin pooling their knowledge and expertise. We have great hope that with their combined insights, we’ll see breakthroughs in science in this area. This will yield new treatments that will give people with Down syndrome better sleep, from early childhood to adulthood, which will be a foundation for much healthier and longer lives.”
For more information, please see DSSRN’s website, and if you wish to stay in contact for updates, please fill out the form here: https://dssrn.org.uk/contact
Queries for the Down Syndrome and Sleep Research Network can be directed to: info@dssrn.org.uk
An open letter to MPs about the Assisted Dying Bill
from a parent in the DS Community
We have been encouraging people to write to their MPs about the Assisted Dying Bill before they vote on it for the final time, as it is quickly moving towards becoming law in the UK. The next debate at Report stage is due Friday 13th June. The 3rd reading vote is likely to be 20th June or even into early July.
When writing to your MP, your personal stories and insights matter more than you might know. A supporter who is a mother of a child with Down syndrome has shared this moving letter with us, which we are posting here. We hope it will inspire you to share your own story too with your own MP.

“Dear [Member of Parliament],
I am writing to you about the Terminally Ill Adults (End of Life) Bill introduced by MP Kim Leadbeater, and am asking urgently that you vote against this bill. I would like to share with you why it matters personally to me, and what worries me most about the direction we are headed in with this Bill.
When my daughter was born with Down Syndrome I was uncertain of what our lives would look like going forward. But I was certain that despite the surprise and adjustment of having a diagnosis at birth, it was better than having a prenatal diagnosis. Maybe I could have prepared better, or taken supplements proven to help babies with DS prenatally if I had known. But I also would have faced enormous pressure about the value of her life. The medical community proves over and over that it does not want people with Down Syndrome to live. A staggering percentage are not given a chance at life because they are aborted. The first thing expectant mothers are offered when they receive a prenatal diagnosis is an abortion.
This is a population of people that light up the world with their smiles, their joy, their kindness. Yet they had to beat the odds just to be born. But if they are lucky enough to be welcomed into their very lucky families, they are not welcomed so readily into society. I have to fight for my daughter to receive adequate medical care … there is nothing wrong with her, but the biochemistry of individuals with Down Syndrome is unique, and doctors often don’t want to take the time to research or educate themselves on the best care for this vulnerable population.
Now this precious group of people who actually survived past the womb despite persecution are facing the same persecution in adulthood. It is naive to believe that the very same medical community that is so reluctant to let them to be born wouldn’t be empowered by an assisted dying bill to do away with them when it’s convenient.
My little daughter is the heart and soul of our family … at two years old she has been fighting daily to make her milestones with the support and encouragement of her siblings. Her whole life she will have to work hard to keep up with her peers. But no one will surpass her in joy, in kindness, in generosity. But she should not have to fight at every stage of her life because of laws that make her vulnerable rather than protect her.
It is incredibly worrying that we are seeing a bill that doesn’t have any safeguards designed to protect people with Down Syndrome, and it doesn’t seem accidental. I am writing to ask you for the sake of many others like her, please do not give your support to this Bill. Please vote against it, because it will surely become another threat to the lives of people like my daughter.
Your sincerely,
Marie G.”
You can find out who your local MP is here: